Paeds · pain-palliative-and-end-of-life-care
Pain assessment across developmental and cognitive abilities
Also known as Paediatric pain assessment · FLACC and revised FLACC · Faces Pain Scale-Revised · Self-report of pain intensity in children · Pain assessment in cognitive impairment · NCCPC and non-verbal pain tools · Pain as the fifth vital sign
Fellowship-level approach to measuring a child's pain honestly across every age and ability: self-report as the gold standard from about four years with the Faces Pain Scale-Revised and the Numerical Rating Scale from about eight years; behavioural observation with FLACC for the two-month to seven-year-old who cannot self-report; individualised observational tools (revised FLACC, Non-communicating Children's Pain Checklist) for children with cognitive impairment or communication disability; COMFORT-behaviour in the PICU; the developmental and cognitive logic that picks the right tool; the traps that undertreat pain (the quiet child, the paralysed child, the child whose behaviour has habituated); and the ANZ, UK and North American standard that pain is the fifth vital sign, reassessed after every intervention and documented in the chart.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-year-old is brought to the emergency department after a scald and lies still and silent on the trolley while the team prepares to clean the burn. A registrar glances over, sees no crying, and writes "comfortable." An hour later the nurse scores the child with FLACC and gets seven out of ten, and morphine is given that should have been given at the door. That gap — between the pain a child is in and the pain the team records — is what this page exists to close. The cleaning and the dressing of the burn live on another page. What lives here is the disciplined, repeatable measurement of a child's pain across every age and every ability, because pain that is not measured is pain that is not treated. [2]
Pain assessment is the act of assigning a reproducible intensity score to a child's pain using a validated instrument matched to their developmental age and communication ability, recording it as a routine observation, and acting on it. [4] Two ideas hold the field together. The first is that self-report is the gold standard: whenever a child can understand the task and communicate an answer, their own rating of their pain is the measure you act on, and observational tools are a fallback that estimates pain only for those who cannot tell you. The second is the developmental and cognitive match: a Faces scale handed to a three-year-old, a generic FLACC applied to a child with dystonia, or a COMFORT score read in isolation on a paralysed child are all the same mistake in different clothing — a good tool used on the wrong patient. [6]
The discipline carries three obligations. Assess with the right tool, reassess after every intervention, and document so that the next clinician inherits a trajectory rather than a single number. Pain is the fifth vital sign, and the pages on neonatal pain, procedural pain, and acute and chronic pain management build on the scores you produce here. [2]
Classification
Classify the assessment task by how the child can communicate, by where the child sits developmentally, and by what confounds the measurement, because those three axes decide the instrument. [4]
The first axis is the communication channel. A self-report tool takes the rating from the child's own answer, and it is the correct choice for any verbal child who can map an internal state onto the scale. An observational or behavioural tool infers pain from what the child does — face, legs, cry, consolability — and is the fallback for the pre-verbal, the frightened, the sedated, and anyone who cannot or will not answer. A physiological tool reads heart rate, blood pressure and oxygenation, but these alone are noisy and are used as supporting signals inside composite tools rather than as standalone measures. [2]
The second axis is developmental age, which is not the same as chronological age. Self-report becomes reliable around four to five years with a Faces scale and matures into the Numerical Rating Scale by about eight years. Below that band, and for any child who cannot understand the abstract mapping, observation takes over. [4] [5]
The third axis is the confounder, and it is the one that hurts children. Cognitive impairment, cerebral palsy and severe movement disorders corrupt the behavioural domains, so the tool must be individualised. [6] Sedation and neuromuscular blockade suppress the very signs observational tools read, so a paralysed child needs an explicit analgesic plan that does not depend on movement. [10] Chronic pain and chronic illness habituate behaviour, so a child in long-standing pain may look calmer than a child in less pain. Classify the confounder before you trust the score.
Epidemiology & Risk Factors
Paediatric pain is common, it is repeatedly under-assessed, and the children most likely to be under-scored are the children least able to speak for themselves. The risk of a misleading assessment is driven by young developmental age, cognitive impairment, critical illness, and chronic or recurrent pain, and it is amplified by staff who reach for a single familiar tool. [2]
Chronic and recurrent pain is far more prevalent than is often assumed. A systematic review of children and adolescents found pooled prevalence estimates for chronic pain in the range of one in four to one in five across studies, with headache, abdominal pain and musculoskeletal pain the most common, and a substantial minority developing persistent pain and disability. [11] Acute and procedural pain is near-universal in hospitalised children, and the children who carry the most procedures carry the most risk of both untreated pain and behavioural sensitisation. [12]
The children at highest risk of being under-scored cluster into three groups. The first is the pre-verbal infant and the young child under about four years, who cannot self-report and depend entirely on observation. [2] The second is the child with cognitive impairment, autism or communication disability, in whom pain is both more common and systematically under-detected; a systematic review and meta-analysis of postoperative pain in children with cognitive impairment found that unrecognised and undertreated pain is the persistent signal across studies, and that individualised tools outperform generic ones. [9] The third is the critically ill or sedated child, in whom the behavioural and physiological signs are pharmacologically suppressed and a low score can sit beside untreated pain. [10]
Pathophysiology
The mechanism that matters for assessment is that pain is a subjective experience, not a behaviour, and behaviour is only an indirect window onto it — a window that age, cognition, sedation and habituation can fog or shutter. Understanding why behaviour and physiology diverge from the underlying pain is what stops you reading a quiet child as comfortable. [2]
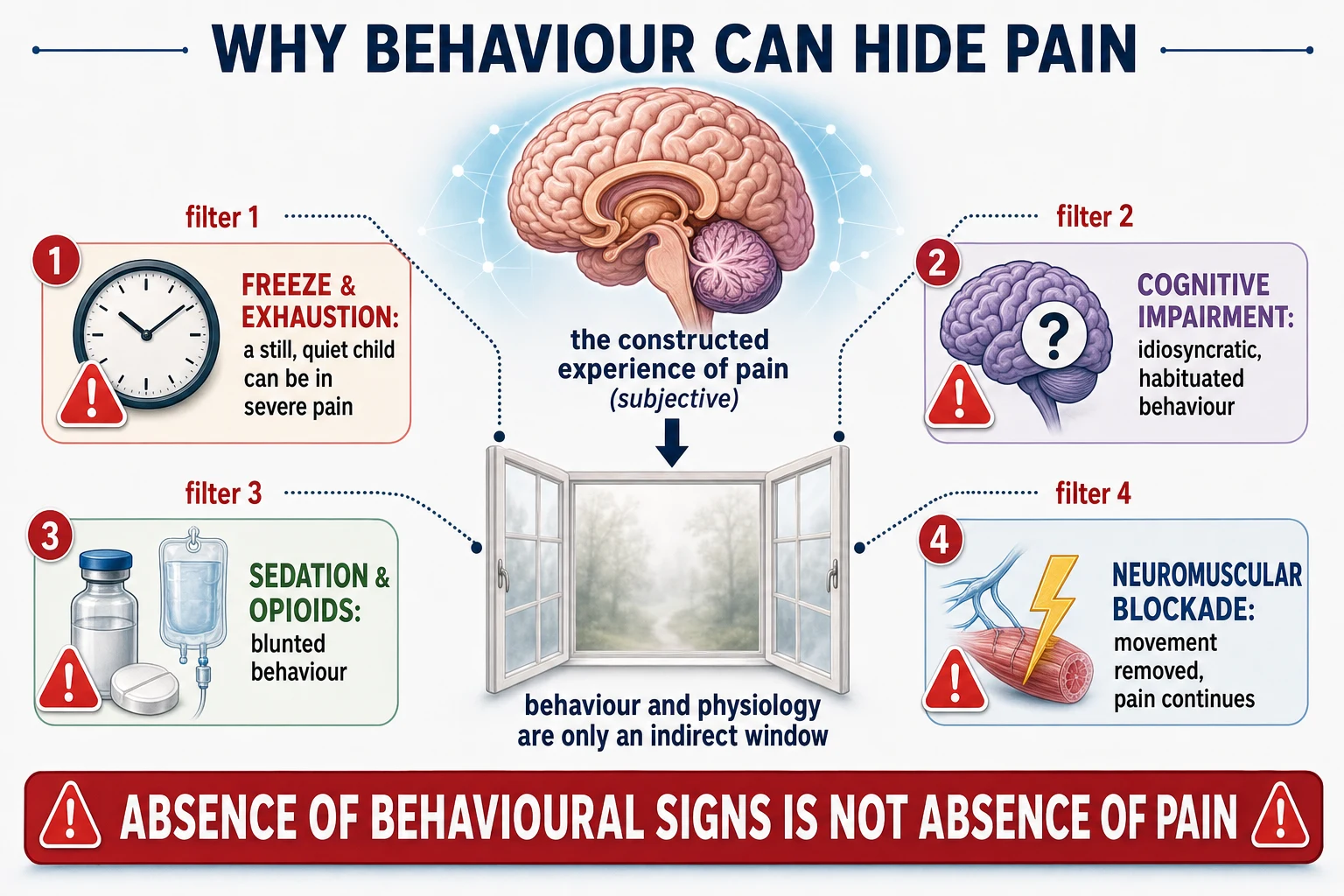
Nociception is the afferent signalling from tissue injury, and pain is the conscious, emotional and cognitive output the brain constructs from that signalling plus context, memory and meaning. Because pain is constructed centrally, two children with identical injury can report and show different pain, and the same child can show different behaviour for the same pain across time. [11] That subjectivity is exactly why self-report is privileged: only the child holds the output, and behaviour is an inference.
Behavioural and physiological signs are the inferences observational tools use, and each has failure modes. A young child in severe pain may freeze rather than cry, may become still rather than thrash, and may withdraw rather than seek comfort — the freeze response that protected the ancestor looks, at the bedside, like comfort. [2] Autonomic signs rise early but habituate fast, so a child in long-standing pain may have a normal heart rate and blood pressure. Sedatives and opioids blunt both behaviour and physiology, and a neuromuscular blocker removes movement entirely while leaving the nociception and the experience intact. [10]
Habituation is the chronic counterpart. A child with longstanding or recurrent pain learns to conserve behaviour, to continue functioning, and to mask distress, so the behavioural score underestimates the experienced pain. This is why baseline change matters more than baseline level: a child whose pain behaviour has moved away from their own normal is in trouble even if the absolute score looks modest. [11]
Clinical Presentation
Pain presents differently at each developmental band, and the band-appropriate signal is the first thing you read. [2]
In the neonate and young infant, pain shows as a coordinated behavioural and physiological burst: brow bulge, eye squeeze, nasolabial furrow, a high-pitched cry, tachycardia and desaturation, with a reduced and disorganised response when the pain is sustained or the infant is preterm or unstable. Neonatal assessment uses validated composite tools (the Premature Infant Pain Profile and equivalents), and that developmental band is covered in depth on the neonatal pain page; the principle that carries forward here is that even the pre-verbal infant has a readable signal, and that signal is scored, not guessed. [2]
In the toddler and preschool child, pain shows as a body — guarding the part, limping, holding still, refusing to move — accompanied by crying, irritability and regression. These children can sometimes point to a Faces scale but cannot reliably use abstract numbers, so a Faces scale is offered where the developmental match holds and observation fills the rest. [4]
In the school-age child, self-report becomes the primary measure. The child can use a Faces scale and, from about eight years, the Numerical Rating Scale, and they can localise and describe the pain. The trap in this band is the frightened or withdrawn child who under-reports to avoid a needle, or who freezes; a self-report is accepted but read alongside behaviour. [5]
In the adolescent, the Numerical Rating Scale is the standard self-report, and the adolescent can describe quality and timing. The risk shifts to under-reporting driven by stoicism, fear, distrust, or a wish to protect a parent, and to chronic and recurrent pain syndromes that present as functional disability as much as as nociception. [11]
In the child with cognitive impairment or communication disability, the signal is idiosyncratic and individual. Vocalisation changes, grimacing, arching, rocking, self-injury, abrupt changes in tone or sleep, and withdrawal may all be pain, and the parent or usual carer is the expert on what this particular child's pain looks like. The generic behavioural tool misreads these signs, so the assessment is individualised. [6] [9]
Differential Diagnosis
The differential of "this child's behaviour has changed" is short, and each item changes whether you are measuring pain or something else. [2]
The first alternative is distress without nociception — fear, anxiety, separation, hunger, a wet nappy, a full bladder, or the unfamiliar environment of hospital. Distress is real and deserves comfort, but treating it as pain and giving an opioid is both an assessment failure and a medication risk, so the behavioural and self-report data are read alongside the context, and reversible non-pain drivers are addressed first or in parallel. [12]
The second is delirium and agitation in the critically ill or postoperative child, where disordered attention and perception produce behaviour that a pain score alone will misread; in the PICU, pain and sedation are assessed together so that an agitated, under-sedated child is not simply labelled as in pain. [10]
The third is neurological change masquerading as behaviour — a dystonic storm, a seizure, raised intracranial pressure, or a movement disorder — which is especially relevant for the child with cerebral palsy or a neurodisability, and which the individualised tool and the carer's account help to separate from pain. [9]
The fourth is habituation, already described, in which a child in longstanding pain shows less behaviour than the pain warrants. The discipline in every case is the same: keep pain on the differential, score it with the right tool, and weigh the result against the child's baseline and the confounders rather than discarding it on the strength of an alternative. [11]
Clinical & Bedside Assessment
At the bedside, run a short, structured assessment in four steps that takes under a minute and prevents most of the under-scoring this page exists to prevent. [2]
THE FOUR-STEP BEDSIDE PAIN ASSESSMENT
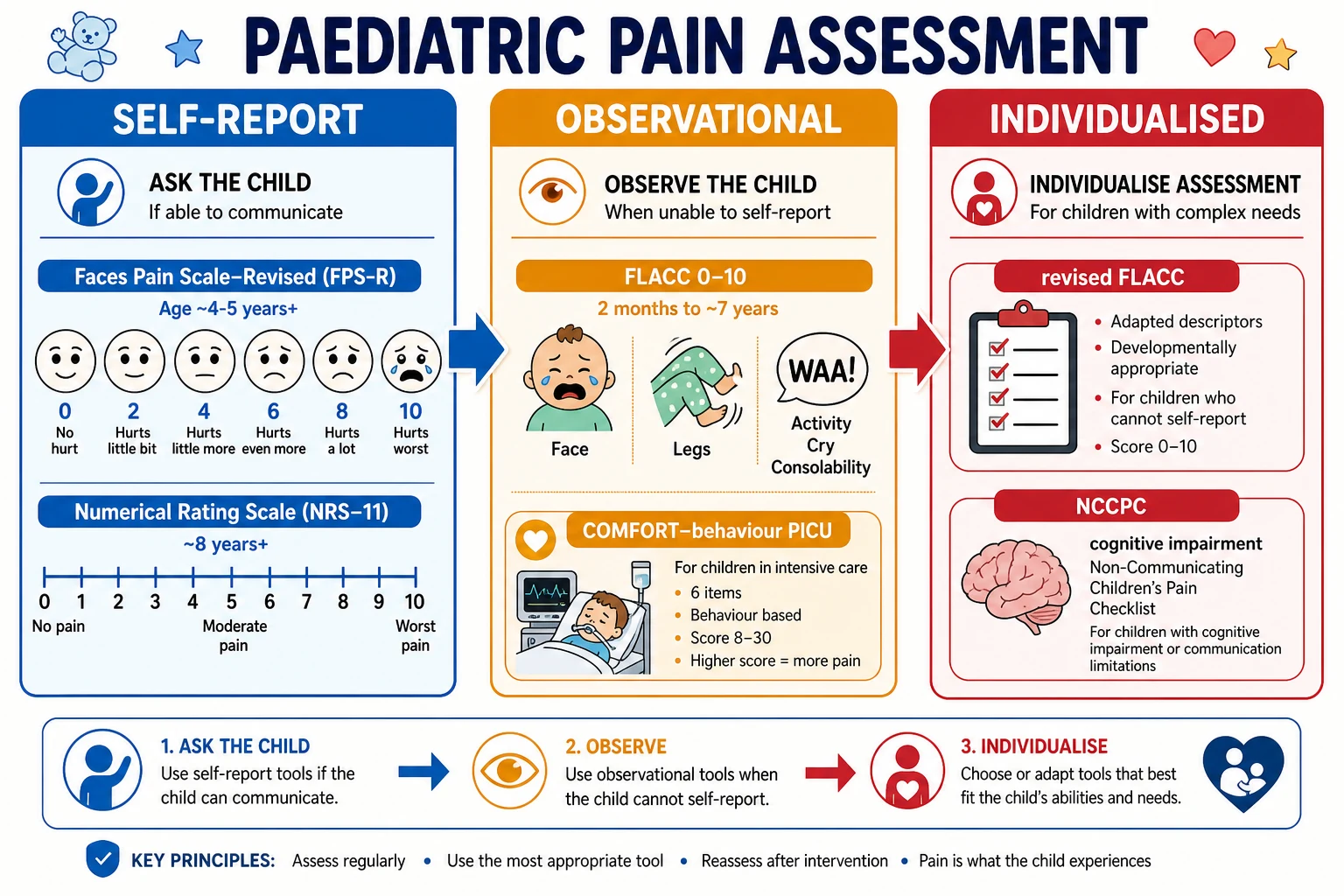
The first step is to ask the child. Whenever the child can understand the task, take their self-report as the primary measure. Offer the Faces Pain Scale-Revised to the four-to-five-year-old upward, and the Numerical Rating Scale to the eight-year-old upward, using language the child understands and watching for the frightened child who under-reports. [3] [5]
The second step is to observe when self-report is not possible. For the infant and the child under about seven years who cannot or will not self-report, score with FLACC, summing Face, Legs, Activity, Cry and Consolability for a total out of ten, and read the score against the clinical context rather than in isolation. [1] [2]
The third step is to individualise for disability. For the child with cognitive impairment, autism, cerebral palsy or a movement disorder, replace generic FLACC with the revised FLACC and the Non-communicating Children's Pain Checklist, and ask the parent or usual carer what this child's pain normally looks like and how today differs from baseline. [6] [7]
The fourth step is to reassess and document. Treat the score as a vital sign recorded in the chart, recheck it after every analgesic intervention against the response you predicted, and escalate when the trajectory is wrong. A single score is a snapshot; the trend is the clinical instrument. [2]
Investigations
There are no laboratory investigations that belong to pain assessment as a topic; the "investigations" here are the validated instruments themselves, and choosing among them is the skill. [4]
The self-report instruments are the Faces Pain Scale-Revised and the Numerical Rating Scale. The Faces Pain Scale-Revised uses six gender-neutral line-drawn faces progressing from no pain to most pain, scored 0 to 10 in two-point steps, validated for children from about four to five years and widely used across childhood and adolescence. [3] A systematic review of faces scales confirmed that the revised scale is among the best-validated and most preferred, and that the common error is allowing the youngest children to confuse the faces with emotion rather than pain intensity, which is why the scale is matched to developmental age. [4] The Numerical Rating Scale asks the child to rate pain from 0 to 10; datasets supporting its use established that it is reliable and preferred from about eight years, and that it should not be routinely used below that age where younger children cannot handle the abstract number-to-feeling mapping. [5]
The observational instruments begin with FLACC. Five categories — Face, Legs, Activity, Cry, Consolability — are each scored 0, 1 or 2 and summed to a total of 10, and the tool was developed and validated for scoring postoperative pain in young children. [1] A systematic review of the FLACC scale across infants and children found moderate to good reliability and validity and good feasibility, with the consistent limitation that the Legs and Activity domains are corrupted by pre-existing movement disorders and that the tool can under-detect pain in the cognitively impaired and the habituated child. [2]
The individualised instruments are the revised FLACC and the Non-communicating Children's Pain Checklist. The revised FLACC retains the FLACC structure but allows the assessor to add individualised, parent-described behaviours under each category, and it demonstrated improved reliability and validity for pain assessment in children with cognitive impairment. [6] The Non-communicating Children's Pain Checklist, validated in its postoperative version, scores seven domains of behaviour over a short observation window for non-verbal children with cognitive impairment, and a head-to-head comparison of tools in this population confirmed that individualised instruments outperform generic ones in clinical utility. [7] [8]
The critical-care instrument is COMFORT-behaviour. The COMFORT scale was built for sedation assessment in the PICU, and the behavioural subset can be used to assess pain; a study of sedation assessment showed that using the COMFORT behaviour scale improved sedation assessment, and the scale is read with the explicit caveat that pain and sedation overlap and that a paralysed child must not be judged comfortable on a behavioural score alone. [10]
Self-report
Ask the child
- Faces Pain Scale-Revised: 6 faces, 0-10, from ~4-5 years
- Numerical Rating Scale 0-10: reliable and preferred from ~8 years
- Gold standard when the child understands the task
- Watch for under-reporting in the frightened or stoical child
Observational
Watch the child
- FLACC: Face, Legs, Activity, Cry, Consolability, total 0-10
- Validated 2 months to ~7 years, acute and postoperative pain
- Fallback when self-report is impossible
- Misreads movement disorders and habituated behaviour
Individualised
Match the child
- Revised FLACC: add parent-described behaviours
- NCCPC: 7 domains for non-verbal cognitively impaired children
- Essential for cerebral palsy, autism, cognitive impairment
- Baseline change matters more than baseline level
Management — Resuscitation
The resuscitation question in this topic is the immediate response to unrecognised or under-recognised severe pain, and to the assessment situations in which a score cannot be trusted. [2]
A child who arrives in severe pain — the burn, the fracture, the sickle-cell crisis, the surgical abdomen — is assessed and given analgesia without waiting for a perfect score. In the verbal child the self-report anchors the urgency; in the pre-verbal or cognitively impaired child a behavioural score plus the clinical context justifies immediate analgesia, because the cost of waiting on a precise number is prolonged, sensitising pain. The pharmacology of that analgesia lives on the acute pain management page; the assessment principle is that severe pain is itself the indication, and a provisional score supports rather than gates the first dose. [2]
The second resuscitation situation is the paralysed or deeply sedated child in the PICU. Neuromuscular blockade removes the movement and much of the behaviour that FLACC and COMFORT depend on, so a behavioural score cannot be the sole basis for analgesia. These children receive an explicit, scheduled analgesic plan that matches the anticipated noxious stimulus, with the behavioural and physiological signs read as supportive rather than decisive, and with the plan revisited as sedation lightens. [10]
Management — Definitive & Stepwise
The definitive management of assessment is a layered, repeatable cycle that begins when a child enters care and ends when the pain has resolved or stabilised, documented as a trend. Build it deliberately, in this order. [2]
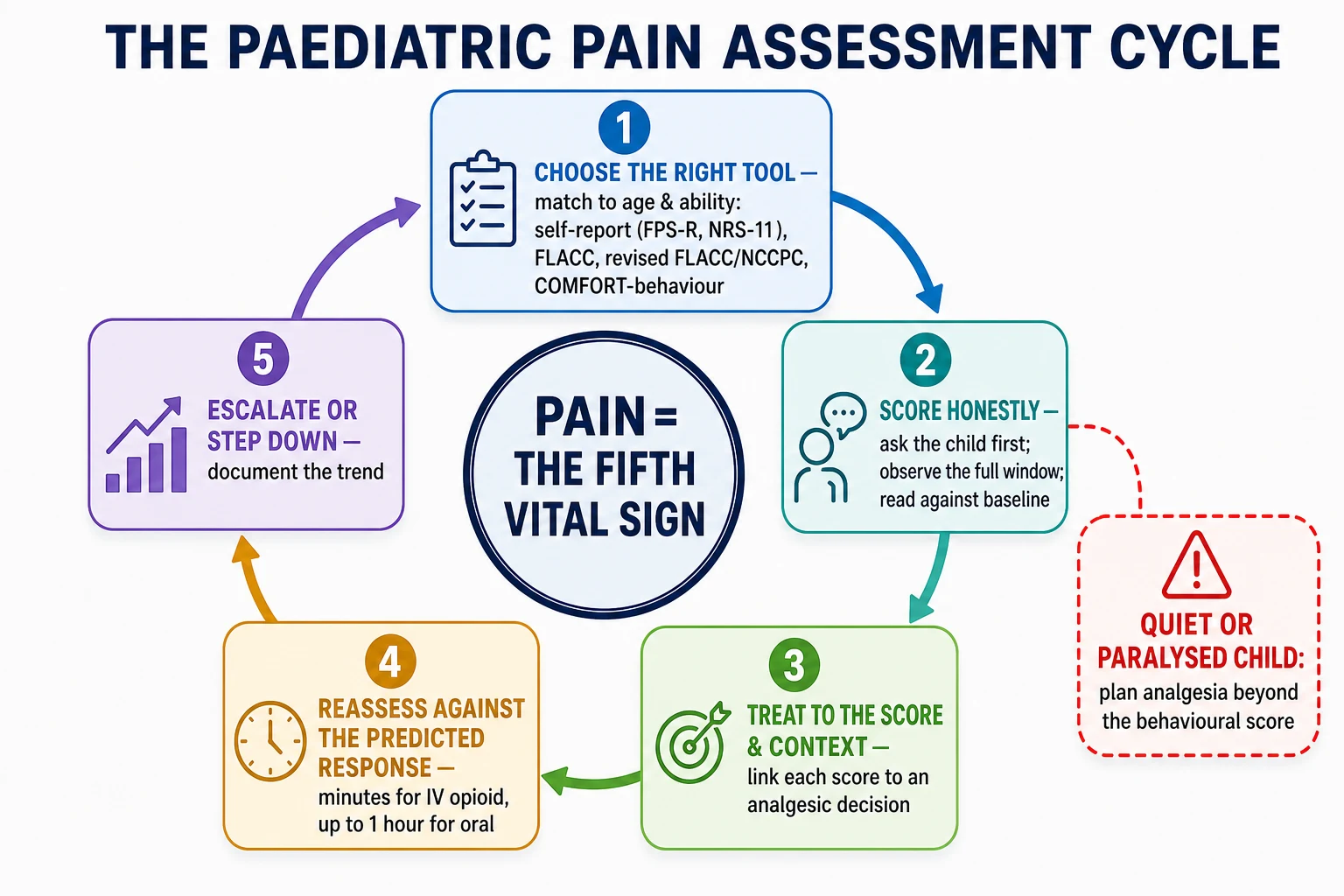
The first step is to choose the right instrument for this child at this moment. Decide on developmental age and communication ability: self-report for the verbal child who understands the task, FLACC for the two-month to seven-year-old in acute pain, the revised FLACC or the Non-communicating Children's Pain Checklist for the cognitively impaired child, and COMFORT-behaviour in the PICU. Naming the choice in the chart makes the assessment auditable and exposes a mismatch. [4] [6]
The second step is to score honestly. Take the child's self-report without leading them, observe for the full window the behavioural tool requires, and resist the pull of the impression. In the cognitively impaired child, ask the carer to score against the child's own baseline, because a change from that baseline is the most sensitive signal available. [9]
The third step is to treat to the score and the clinical context, escalating analgesia for moderate and severe pain and using the non-pharmacological and procedural-comfort measures that reduce the nociceptive load. The pharmacology lives on the acute pain management page; the assessment contract is that the score drives a decision, and that no score is recorded without a corresponding plan. [12]
The fourth step is to reassess against the response you predicted. After the analgesic, recheck the score at the interval appropriate to the drug — minutes for intravenous opioids, up to an hour for oral agents — and compare it with the reduction you expected. A pain that has not moved asks why: is the dose too small, the route wrong, the diagnosis incomplete, or is the behaviour being driven by fear or delirium rather than nociception? The reassessment converts a measurement into a clinical argument. [2]
The fifth step is to escalate or step down along the trend. A falling score justifies stepping down safely; a flat or rising score after a reasonable dose triggers a senior review, a reconsideration of the cause, and a change of plan. The cycle is documented so that the trend, not the last number, is what the next clinician inherits. [11]
Specific Subtypes & Scenarios
Each developmental and clinical scenario needs its own instrument, and the fellow is examined on the match. [4]
For the self-reporting school-age child and adolescent, the Faces Pain Scale-Revised and the Numerical Rating Scale are the standard pair. From about eight years the Numerical Rating Scale is reliable and preferred, and it should not be used below that age. The Faces scale remains useful across the band and as a bridge for the younger or anxious child. [3] [5]
For the infant and the young child under about seven years, FLACC is the workhorse, applied in acute, postoperative and procedural settings and read with the caveat that it can under-detect pain in the habituated child. [1] [2]
For the child with cognitive impairment or communication disability, the revised FLACC and the Non-communicating Children's Pain Checklist replace generic FLACC. The revised FLACC improves reliability and validity in this population by folding in individualised behaviours, and the Non-communicating Children's Pain Checklist, validated in its postoperative version, gives a structured seven-domain observation for the non-verbal child. A comparison of clinical utility across tools in this population confirmed that the individualised instruments serve these children best. [6] [7] [8]
For the critically ill child in the PICU, COMFORT-behaviour is used alongside an explicit sedation assessment, because pain and sedation overlap and a behavioural score can reflect either; a child who is under-sedated may be agitated rather than in pain, and a child who is paralysed cannot behave at all. [10]
For the child with acute procedural pain, assessment is paired with the comfort measures that reduce the noxious input and with the child-life support that lowers the distress that behavioural tools can mistake for pain; the procedural pain page owns the comfort bundle, and this page owns the score that proves it worked. [12]
Complications & Pitfalls
The complications of poor pain assessment are immediate and cumulative, and most are preventable. [2]
The first pitfall is defaulting to observation when the child can self-report. A frightened seven-year-old handed a FLACC instead of being asked is assessed less well, not more, and the staff member's habit overrides the child's voice. Self-report is taken first, always. [5]
The second is the quiet child. Stillness, withdrawal, a flat affect and sleep can each mark severe pain, and the freeze response in particular is misread as comfort. When the clinical situation implies pain, the score is read against the context and the child is treated. [2]
The third is the wrong tool for the disability. Generic FLACC applied to a child with cerebral palsy or a movement disorder is corrupted at the Legs and Activity domains, and the result is systematic under-detection. The individualised tool and the carer's baseline are the correction. [9]
The fourth is the sedated or paralysed child. Sedation and neuromuscular blockade suppress the behavioural and physiological signs, so a low score can sit beside untreated pain. These children carry an explicit analgesic plan that does not depend on movement. [10]
The fifth is the single assessment. A score recorded once and never revisited is a measurement without a response, and it neither confirms that analgesia worked nor exposes that it did not. The reassessment is the assessment. [2]
The long-term complication of repeated under-assessment is sensitisation, needle fear and healthcare avoidance, and a contribution to the chronic pain trajectory that affects a substantial minority of children and adolescents. [11] [12]
Prognosis & Disposition
The prognosis of pain is more modifiable than almost any other paediatric outcome, and the modifiability turns on assessment, because assessment is the gate to treatment. A child whose pain is measured with the right tool, treated to the score, and reassessed against the predicted response does better in the moment and over time; a child whose pain is under-scored is under-treated, and under-treated acute pain sensitises the child for the next procedure and feeds the chronic pain trajectory. [11]
For acute pain the disposition follows the trend. A falling score with a working plan supports discharge with oral analgesia and clear safety-netting; a flat or rising score keeps the child in for review of the cause and the plan. For procedural pain the disposition is a documented reassessment and a note on what worked for the next visit, because the memory of unmanaged pain is the strongest predictor of distress at the next procedure. [12]
For the child with cognitive impairment the disposition is an individualised plan the family can carry forward, because the carer's ability to read baseline change is what protects the child between visits. For chronic and recurrent pain the disposition is a multimodal plan and a trajectory of function as well as of intensity, because recovery is measured in participation and school attendance, not only in a number out of ten. [11]
Special Populations
The assessment approach is tailored, not templated, for each special population, and the tailoring is examined. [9]
The child with cognitive impairment or communication disability is the population this page is built around. Generic behavioural tools under-detect their pain, so the revised FLACC and the Non-communicating Children's Pain Checklist are the standard, individualised with the carer's account of the child's baseline pain behaviour. A systematic review of postoperative pain in children with cognitive impairment found under-recognition to be the persistent failure across studies, and individualised assessment to be the consistent remedy. [6] [7] [9]
The critically ill or technology-dependent child in the PICU is assessed with COMFORT-behaviour within an explicit sedation-and-pain framework, with the paralysed child given an analgesic plan that does not depend on behaviour. [10]
The Aboriginal and Torres Strait Islander child, and the migrant, refugee or asylum-seeking child, may face language, cultural and trust barriers that distort both self-report and the team's interpretation of behaviour. A trained interpreter, culturally safe communication, and attention to past experiences of pain and healthcare protect the assessment from these distortions. [2]
The child with chronic or recurrent pain is assessed for function and trajectory as well as intensity, because a single score under-represents longstanding pain that has habituated behaviour; the trend and the functional impact are the measures that matter. [11]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric pain assessment is strong on the validity and reliability of the major tools and on the harm of under-assessment, and the regional guidelines agree on the principle that pain is the fifth vital sign while differing on operational detail. [4]
The Faces Pain Scale-Revised, validated toward a common metric in paediatric pain measurement, and the systematic reviews of faces scales and of the FLACC scale, establish the self-report and observational workhorses. [3] [4] [2] The revised FLACC and the Non-communicating Children's Pain Checklist, with the head-to-head comparison of clinical utility, establish the individualised approach for cognitive impairment, and a recent meta-analysis confirms that under-detection in this population remains the signal failure. [6] [7] [8] [9] The Numerical Rating Scale datasets set the age threshold for reliable self-report, and the COMFORT-behaviour work sets the critical-care standard. [5] [10]
Regionally, the Royal Children's Hospital Melbourne guideline on pain assessment and measurement is the standard reference in ANZ and embeds the developmental tool-selection logic and the fifth-vital-sign principle, built on the validated tools the literature establishes. [2] In the United Kingdom, the Royal College of Nursing guidance on the recognition and assessment of acute pain in children and the RCPCH framework set the equivalent standard, and the National Health Service embeds paediatric pain assessment in ward observations, again using the validated self-report and observational instruments. [4] In North America, the American Academy of Pediatrics guidance on paediatric palliative care and pain management, and the WHO 2020 guideline on the management of chronic pain in children, set the international benchmark, with the WHO emphasising that assessment must be matched to the child's developmental stage and communication ability. [9] [11] The areas of genuine controversy are narrow: the exact age at which a child can use the Numerical Rating Scale, the degree to which physiological signs add value inside composite tools, and the optimal frequency of reassessment in stable and chronic settings — and on all three the conservative answer is to match the tool to the individual child rather than to a unit-wide default.
Exam Pearls
PAINS
Anticipate the pain the clinical situation implies — a burn, a fracture, an incision, a paralysed PICU patient — before you reach for a tool
Take the child's self-report first: FPS-R from ~4-5 years, NRS-11 from ~8 years; it is the gold standard when the child understands the task
Switch to revised FLACC or NCCPC for cognitive impairment; fold in the carer's account of this child's own baseline pain behaviour
Score with a validated tool and document it as the fifth vital sign, so the next clinician inherits a trajectory not a guess
Reassess after every analgesic against the reduction you predicted; a score that has not moved asks why
The number that traps the unwary is the behavioural zero in a context that implies pain. A FLACC of two in a child with a fresh scald, a fractured femur or a surgical incision is not reassurance; it is a measurement error waiting to be corrected by context, a different tool, and an analgesic plan. [2]
The one-line fellowship answer: ask the child first with a developmentally matched self-report scale, observe with FLACC when they cannot self-report, individualise with the revised FLACC or the Non-communicating Children's Pain Checklist for cognitive impairment, and treat every score as the fifth vital sign — reassessed after every analgesic, documented as a trend, and read against the clinical context rather than in isolation. [3] [6] [10]
References
- [1]Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs, 1997.PMID 9220806
- [2]Crellin DJ, Harrison D, Santamaria N, Babl FE Systematic review of the Face, Legs, Activity, Cry, Consolability scale for assessing pain in infants and children: is it reliable, valid, and feasible for use? Pain, 2015.PMID 26207651
- [3]Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B The Faces Pain Scale-Revised: toward a common metric in pediatric pain measurement. Pain, 2001.PMID 11427329
- [4]Tomlinson D, von Baeyer CL, Stinson JN, Sung L A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics, 2010.PMID 20921070
- [5]von Baeyer CL, Spagrud LJ, McCormick JC, Choo E, Neville K, Connelly MA Three new datasets supporting use of the Numerical Rating Scale (NRS-11) for children's self-reports of pain intensity. Pain, 2009.PMID 19359097
- [6]Malviya S, Voepel-Lewis T, Burke C, Merkel S, Tait AR The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr Anaesth, 2006.PMID 16490089
- [7]Breau LM, Finley GA, McGrath PJ, Camfield CS Validation of the Non-communicating Children's Pain Checklist-Postoperative Version. Anesthesiology, 2002.PMID 11873023
- [8]Voepel-Lewis T, Malviya S, Tait AR, Merkel S, Foster R, Krane EJ, Davis PJ A comparison of the clinical utility of pain assessment tools for children with cognitive impairment. Anesth Analg, 2008.PMID 18165556
- [9]Pizzinato A, Liguoro I, Pusiol A, Cogo P, Palese A, Vidal E Detection and assessment of postoperative pain in children with cognitive impairment: a systematic literature review and meta-analysis. Eur J Pain, 2022.PMID 35271756
- [10]Ista E, van Dijk M, Tibboel D, de Hoog M Assessment of sedation levels in pediatric intensive care patients can be improved by using the COMFORT "behavior" scale. Pediatr Crit Care Med, 2005.PMID 15636661
- [11]King S, Chambers CT, Huguet A, MacNevin RC, McGrath PJ, Parker L, MacDonald AJ The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain, 2011.PMID 22078064
- [12]Taddio A, Shah V, McMurtry CM, Lang E, MacDonald NE, Constantin K A Systematic Review and Meta-Analysis of the Effectiveness of Procedural Interventions for Reducing Distress During Vaccine Injections. Clin J Pain, 2026.PMID 41880242