Paeds · investigations-procedures-and-technology
Procedural pain: topical anaesthesia, preparation, distraction and non-pharmacological support
Also known as Procedural pain management in children · Paediatric procedural analgesia · Needle pain reduction · Comfort bundle for procedures · Ouchless care · Child-life and distraction
Fellowship guide to managing procedural pain in infants and children with a multi-modal comfort bundle. Covers why untreated procedural pain is harmful and ethical fail, the four layers of the comfort bundle (preparation and child life, topical anaesthesia, sweet taste and breastfeeding, distraction and comfort positioning), the agents and their timings (EMLA lidocaine-prilocaine 60 minutes and its methaemoglobinaemia risk in infants under three months, amethocaine 4% gel 30 to 45 minutes, liposomal lidocaine 4%, oral sucrose 24% at 0.1 to 2 mL given two minutes before and never as mL per kg, breastfeeding during the procedure), how each works (sodium-channel blockade in skin nociceptors, endogenous opioid and dopamine activation by sweet taste, gate-control and attentional modulation by distraction), the age- and procedure-specific approach from the neonate to the needle-phobic adolescent, the avoidance of forceful hold-down restraint, the HELPinKIDS and Cochrane evidence base, and the ANZ, UK and North American guideline differences. Woven throughout is the principle that comfort is a standard of care layered around every needle and painful procedure, not an optional extra.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-year-old in the emergency department who needs a cannula, backing into the corner the moment the tourniquet appears. Picture the neonate on the ward having a heel lance for a blood gas. In both, the question the team must answer is the same — how do we make this needle hurt as little as possible, and how do we stop it becoming a memory the child carries for life. That is the territory this page owns. [1] [9]
A painful procedure is any planned clinical act that is expected to cause tissue injury and pain — venepuncture, cannulation, intramuscular vaccination, a heel lance, suturing a laceration, lumbar puncture, dressing a burn, or removing a chest drain. Procedural pain is the pain the child experiences during that act, and procedural comfort is the deliberate, multi-modal effort to reduce that pain and the fear around it. The interventions fall into four families: pharmacological-topical agents that numb the skin, sweet-taste and oral measures such as sucrose and breastfeeding, psychological preparation and child-life support, and behavioural measures such as distraction and comfort positioning. [1] [11]
What makes paediatric procedural pain a distinct skill is that the child cannot always cooperate, the response to pain and fear changes with development, and a single unmanaged painful procedure can rewire how a child encounters healthcare for years. The fellowship skill being tested is reading the child and the procedure, choosing and timing the right combination of layers, and refusing to use a needle on an unprepared, under-analgesed child when time allows. [10] [1]
Classification
Sort the comfort measures by the limb of the pain response they act on, because a single layer is rarely enough and the layers combine by design. [1] [11]
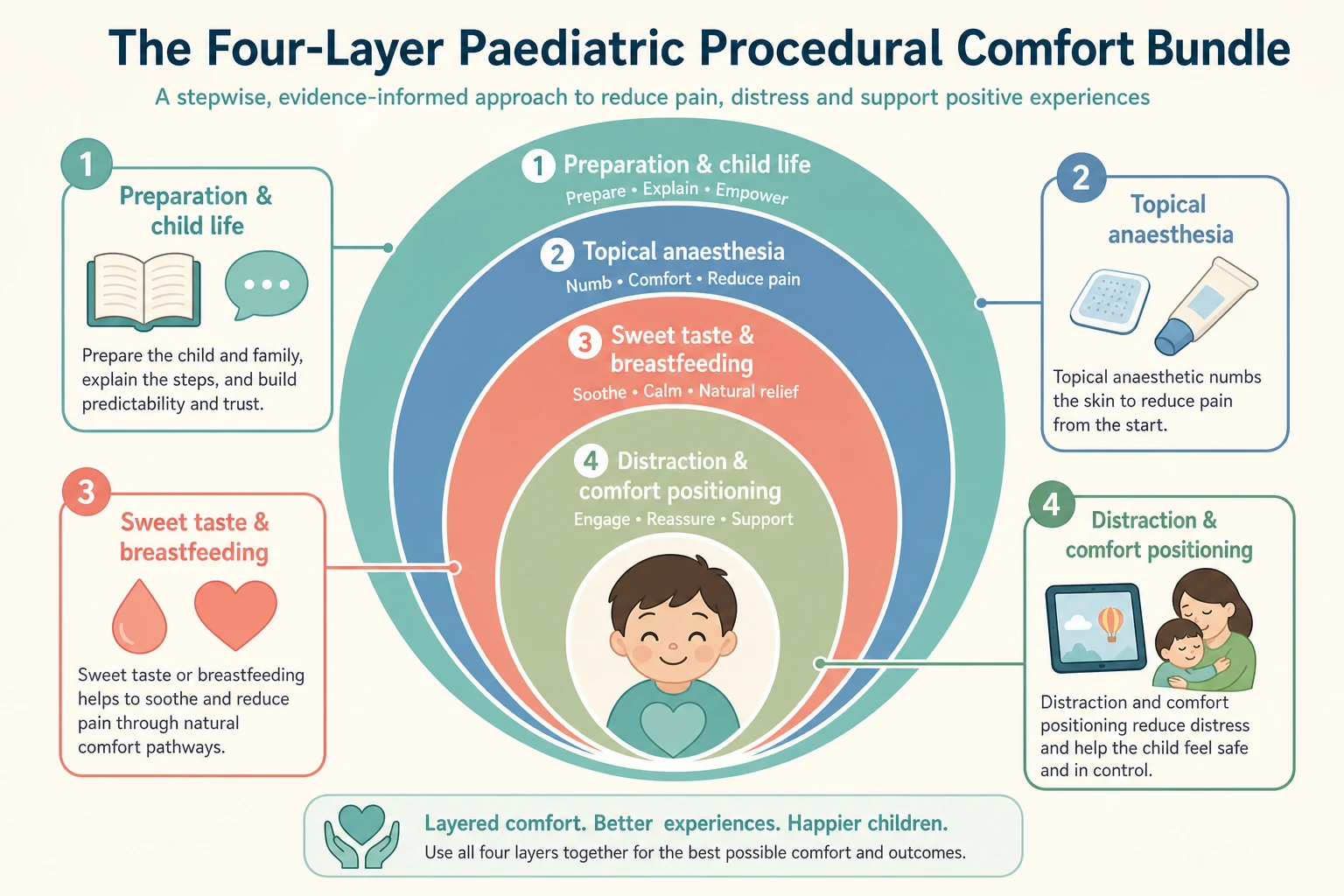
By pharmacological-topical agents, a topical anaesthetic numbs the skin at the procedure site before the needle passes. The two workhorses are EMLA, a eutectic mixture of lidocaine 2.5% and prilocaine 2.5% that needs at least 60 minutes under an occlusive dressing, and amethocaine 4% gel (Ametop), an ester that works faster at 30 to 45 minutes and is the safer choice in neonates and young infants. Liposomal lidocaine 4% (LMX4) is a useful amide alternative that needs about 30 minutes without occlusion. [2] [5]
By sweet-taste and oral measures, a small volume of a sweet solution or breastfeeding reduces pain in infants through endogenous opioid and dopamine release. Oral sucrose 24%, 0.1 to 2 mL given about two minutes before and again as the procedure starts, is the standard for neonates and young infants; breastfeeding during the procedure is at least as effective and often more so. These measures work best in the first year and lose effect as the child grows. [3] [4]
By psychological preparation and child-life support, an honest, developmentally-appropriate explanation of what the child will feel, what it is for, and what will help, delivered before the procedure, lowers fear and improves cooperation. A child-life specialist uses play, dolls, books and coping plans to give the child a sense of control, and the preparation is a treatment in its own right, not a courtesy. [9] [10]
By behavioural measures, distraction and comfort positioning direct the child's attention away from the needle and keep the child feeling safe. Distraction is matched to age — bubbles, singing or a parent reading for the toddler, a video or game on a tablet for the preschool and school-age child, and immersive virtual reality for the older cooperative child. Comfort positioning replaces the lying-flat hold-down with an upright chest-to-chest hug on a parent's lap, which paradoxically gives the operator better access and the child more control. [7] [8]
The numbers that anchor your viva
Epidemiology & Risk Factors
Needle procedures are among the commonest events in a child's healthcare — vaccination schedules alone deliver more than a dozen injections before school age, and a hospitalised child may face cannulation, blood tests and dressing changes daily. The default for decades was to perform them with little or no analgesia, and under-treatment of paediatric procedural pain remains the failure mode the comfort bundle is designed to correct. [9] [10]
The risk of a poorly managed procedure is a memory, not just a moment. A child who experiences uncontrolled needle pain develops needle fear and, in a significant minority, needle phobia that persists into adulthood, driving vaccine refusal, avoidance of healthcare, and the vasovagal fainting that closes the loop. The earlier and the more painful the early experiences, the stronger the learned fear, which is why the first needle matters disproportionately. [11] [1]
Certain children are at higher risk of severe distress and of being under-treated. Young infants cannot report pain and are easily assumed not to feel it. Children with developmental disability, autism or communication impairment may express pain differently or be restrained more often. Children with complex chronic illness undergo repeated procedures and accumulate fear. Needle-phobic children and their parents bring conditioned fear into every encounter. And unaccompanied, frightened or previously-traumatised children lack the buffering presence of a trusted adult. [10] [12]
Pathophysiology
The teaching model runs from the skin nociceptor to the brain's pain neuromatrix, and it rests on the fact that pain is a constructed experience that each layer of the bundle dampens at a different point. [1] [10]
A topical anaesthetic works at the periphery. Lidocaine, prilocaine, tetracaine and the liposomal lidocaines all block voltage-gated sodium channels in the nociceptor endings in the skin, which stops the generation and conduction of the action potential that would carry the needle's signal toward the spinal cord. The agent must reach the dermal nerve plexus in effective concentration, which is why EMLA needs 60 minutes under occlusion and Ametop 30 to 45 minutes — a shorter application is not a weaker version of the same effect, it is no effect at all. [2] [5]
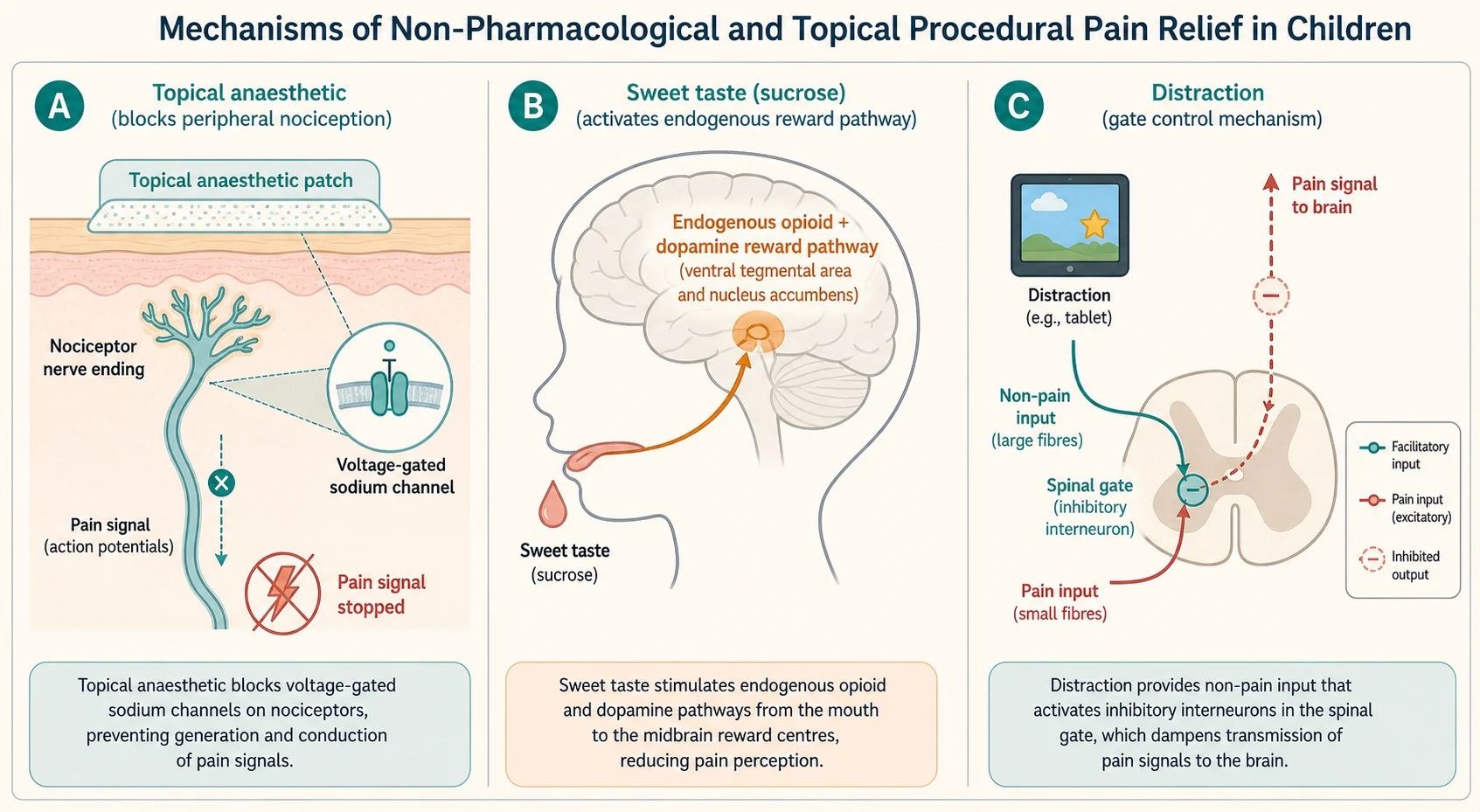
A sweet solution or breastfeeding works through the brain's reward and descending inhibitory systems. The sweet taste on the tongue activates a pathway from the taste buds to the midbrain that releases endogenous opioids and dopamine, which both produces a calming, rewarding effect and engages descending inhibition of the incoming pain signal. The effect is partly but not fully reversed by naloxone, which tells us there is an opioid and a non-opiponent component, and it is strongest in the youngest infants and attenuates with age. [3] [12]
Distraction and comfort positioning work through attention and the gate-control system. Pain is not a faithful readout of tissue damage; it is a constructed experience in which attention, expectation and emotion tune the weight given to the incoming signal. A compelling distraction competes for the attentional resources that would otherwise amplify the pain, and the gate-control model frames this as modulation of the signal at the spinal cord. Comfort positioning and a trusted adult reduce the threat value of the encounter, and a lower threat value means a lower pain experience. [7] [1]
The reason a badly managed first procedure matters so much is fear-memory conditioning. Pain experienced under high threat and low control is encoded as a conditioned fear response, so the next needle is met not with the pain of the needle itself but with the anticipatory fear of the last one. Breaking that loop — by making the first and every procedure as comfortable as possible — is prevention as much as treatment. [11] [10]
Clinical Presentation
The clinical scenarios that prompt a comfort plan are few and well defined, and the first task is to recognise which one you are in, because the bundle is layered differently in each. [9] [10]
The commonest scenario is the planned needle procedure in a child old enough to anticipate it — a vaccination in the clinic, a blood test or cannula in the emergency department, a dressing change on the ward. The child arrives with a mixture of curiosity and fear, and the parent arrives with their own memory of needles, which the child reads off them. The window to prepare, apply topical anaesthesia and set up distraction is before the child sees the tray. [11] [8]
The second is the neonate or young infant who cannot tell you they hurt. A heel lance, a venepuncture or a cannulation in a baby is judged by behavioural and physiological signs — a grimace, a high-pitched cry, a change in heart rate or oxygen saturation — and the trap is to mistake the absence of a complaint for the absence of pain. The comfort plan here is sucrose, breastfeeding or skin-to-skin, containment, and a dummy. [3] [12]
The third is the needle-phobic or previously-traumatised child, who may panic, fight, freeze or faint at the sight of the needle. This child needs more than the routine bundle — extra time, a careful plan, a coping strategy agreed in advance, and, when the fear is severe, formal psychological input or procedural sedation rather than a forceful hold-down. [11] [10]
The fourth is the child needing a procedure that the topical and non-pharmacological layers cannot make comfortable alone — a lumbar puncture, an abscess drainage, a complex dressing change, a fracture manipulation. Here the comfort bundle is the foundation, but it is escalated to formal procedural sedation by a trained team, and the two are complementary, not alternatives. [1] [9]
Differential Diagnosis
The differential at the bedside is not "what is causing the pain" — it is which layers are appropriate for this child and this procedure, in whom each agent is unsafe, and when to escalate beyond the bundle. Frame the decision around four questions and the answer follows. [1] [11]
Routine bundle
default
- Planned needle procedure with time to prepare: vaccination, venepuncture, cannulation
- Child over 3 months with no contraindication to the chosen topical agent
- Parent present and able to hold; child-life and distraction available
- Topical anaesthesia + sucrose or breastfeeding (infant) + distraction + comfort positioning
Neonatal bundle
- Neonate or young infant: heel lance, venepuncture, cannulation
- Ametop (amethocaine 4%) preferred over EMLA to avoid prilocaine methaemoglobinaemia
- Oral sucrose 24% 0.1–2 mL 2 min before; breastfeeding or skin-to-skin; non-nutritive sucking; containment
- Minimise repeated heel lances; cluster care and rest between procedures
Escalate to sedation
- Procedure too painful or distressing for topical + comfort alone: LP, abscess drainage, fracture manipulation
- Severe needle phobia or panic unresponsive to a careful comfort plan
- Child unable to cooperate for a procedure that must be done still
- Formal procedural sedation by a trained team with full monitoring; the bundle is still layered underneath
Do not use this agent
- EMLA in infants under 3 months, preterm babies, or G6PD deficiency — prilocaine methaemoglobinaemia
- Amethocaine in known ester or PABA allergy — use an amide alternative
- Large-volume sucrose or sucrose drawn as mL/kg — give absolute 0.1–2 mL
- Forceful hold-down restraint as a substitute for analgesia and preparation
A second layer of decision is how much time you have. The elective clinic vaccination has time for a full EMLA hour; the emergency-department cannula in a sick child may not, and here Ametop or LMX4 with a faster onset, or a subcutaneous lidocaine wheal for the cooperative older child, is the pragmatic choice. The honest answer to "there was no time" is often "the topical was not applied when the procedure was first anticipated", which is a systems problem the comfort pathway is meant to fix. [9] [6]
Clinical & Bedside Assessment
Assessment before a procedure is short, structured and explicit: it asks about the child, the procedure, the allergies and the time, and it ends with a written comfort plan. The aim is that no child meets a needle unprepared. [9] [10]
Begin with the child: their age and developmental stage, their previous experience of needles, their current anxiety, and whether they have a known needle fear or phobia. Ask the parent how the last procedure went, because a parent's recall of a bad experience is the single best predictor of a difficult one. Note any developmental disability, autism or communication impairment that changes how the child expresses pain and cooperates, and plan extra time and a tailored approach. [11] [10]
Assess the procedure: what it is, how painful it is expected to be, how long it will take, and how still the child must be. A vaccination is brief and superficial; a cannulation needs the hand or arm still for a minute; a lumbar puncture or a fracture manipulation needs far more and points to sedation. The anticipated pain sets how many layers you layer and whether you escalate. [1] [9]
Check the allergies and contraindications that change the topical choice. Ask specifically about local-anaesthetic allergy and para-aminobenzoic acid, because amethocaine is an ester and cross-reacts in ester-sensitive patients. Note G6PD deficiency, preterm birth and age under three months, because each raises the methaemoglobinaemia risk of EMLA and points to Ametop or an amide instead. Confirm there is no broken skin or infection exactly where a topical patch would sit. [2] [5]
The pre-procedure comfort assessment
Child: age, development, prior needle experience, needle fear or phobia, communication needs
Procedure: type, expected pain, duration, how still the child must be — sets how many layers and whether to sedate
Allergies: local anaesthetic, ester/PABA, para-aminobenzoic acid — choose amide vs ester topical
Contraindications: age under 3 months, preterm, G6PD deficiency → avoid EMLA (prilocaine); choose Ametop or amide
Time: how long until the needle? Apply EMLA 60 min or Ametop 30–45 min now if time allows
Write the comfort plan: topical + sweet/oral + distraction + comfort position + caregiver role
Investigations
There is no laboratory panel that precedes a routine comfort bundle, but a small number of bedside checks protect the child from the one serious avoidable harm of topical anaesthesia. The candidate should know what to confirm before the patch goes on and what to watch for after. [2] [10]
Confirm the methaemoglobinaemia risk factors before choosing EMLA. These are age under three months, preterm birth (corrected age), G6PD deficiency, and concurrent exposure to other oxidant agents such as benzocaine, sulphonamides, dapsone or nitrates. A child in any of these groups should receive Ametop or an amide topical instead, because prilocaine metabolism produces the oxidant metabolite that drives methaemoglobinaemia. [2] [5]
Check the skin at the intended site: a topical patch needs intact skin, and an area of eczema, infection or broken skin will both absorb erratically and sting. For a child with a known local-anaesthetic contact allergy, a patch-test history matters, and an amide such as liposomal lidocaine is preferred over an ester where there is ester sensitivity. [5] [6]
During any procedure where the comfort bundle is combined with formal sedation, the monitoring is the sedation team's responsibility — continuous pulse oximetry, heart rate, and a trained observer — and the non-pharmacological layers do not replace that monitoring. The bundle and sedation are layered together, with sedation adding safety and amnesia on top of the comfort already planned. [1] [10]
Management — Resuscitation
The "resuscitation" of a procedural-pain encounter is the recognition and immediate management of the two acute harms that the bundle can cause or fail to prevent: methaemoglobinaemia from a topical anaesthetic, and the vasovagal or anaphylactic reaction of a needle-phobic child. [2] [10]
Methaemoglobinaemia presents within minutes to a few hours of a prilocaine-containing topical as cyanosis that does not improve with supplemental oxygen, a chocolate-brown discoloration of the blood, and a pulse oximetry that sits lower than expected or plateaus around 85 to 90 percent. The level to act on is clinical cyanosis with a raised methaemoglobin fraction (symptomatic thresholds are usually above 20 to 30 percent). Stop the agent, give high-flow oxygen, and treat symptomatic methaemoglobinaemia with methylene blue 1 to 2 mg per kilogram intravenously; a child with known G6PD deficiency may not tolerate methylene blue and needs specialist advice. [2] [5]
Methylene blue (symptomatic methaemoglobinaemia from prilocaine/EMLA)
A vasovagal reaction in a needle-phobic older child or adolescent presents with pallor, sweating, bradycardia and a brief loss of consciousness at or just before the needle. Lay the child flat, raise the legs, give oxygen, and the episode usually resolves within minutes; the prevention for next time is a supine procedure, applied counter-pressure, and, where appropriate, a planned coping or desensitisation strategy. Anaphylaxis to a topical or injected agent is managed in the standard paediatric adrenaline pathway. [11] [10]
The single rule that protects the child from iatrogenic harm is that restraint is never the resuscitation of a distressed encounter. A child held down by force for an elective procedure without adequate analgesia and preparation is being harmed, and the correct response to "they won't hold still" is to stop, prepare, and escalate to sedation where needed — not to add more hands to the hold-down. [9] [10]
Management — Definitive & Stepwise
Once the child, the procedure, the allergies and the time have been assessed, the comfort bundle is applied as an ordered sequence that should run the same way every time: prepare, numb, position, distract, soothe, and then do the procedure calmly. [9] [1]

Prepare the child and parent with an honest, developmentally-appropriate explanation well before the tray appears. Tell the child what will happen, what it is for, and what it will feel like in words they understand — for the young child, "a small pinch that goes away" rather than a false "it won't hurt". Engage child-life where available to use play, dolls and a coping plan, and agree with the child which distraction they will use. Deception destroys trust and worsens the next encounter. [9] [10]
Apply the topical anaesthetic early, because the commonest reason a topical "fails" is that it was not given time to work. Apply EMLA under an occlusive dressing at least 60 minutes before the needle, or Ametop for 30 to 45 minutes, choosing Ametop in the neonate and young infant and avoiding EMLA under three months. Where time is short, LMX4 for about 30 minutes without occlusion, or a subcutaneous lidocaine wheal in the cooperative older child, are the pragmatic alternatives. [2] [5]
COMFORT
Position and soothe the child for the procedure. Replace the lying-flat hold-down with an upright comfort position — a chest-to-chest hug on a parent's lap for the young child, or a supported sitting position for the older child — which gives the operator access while keeping the child in control. For the neonate and young infant, give oral sucrose 24%, 0.1 to 2 mL about two minutes before and again as the needle goes in, or breastfeed during the procedure, and offer a dummy for non-nutritive sucking and swaddled containment. [3] [4]
Distract with something genuinely absorbing and matched to age — bubbles, a song or a parent reading for the toddler; a video or interactive game on a tablet for the preschool and school-age child; and immersive virtual reality for the cooperative older child and adolescent. For the school-age and older child a vibration-and-cold device placed near the injection site exploits gate-control to reduce the pain of a single needle. [7] [8]
Perform the procedure calmly and efficiently, with the parent coached on their role, the distraction running, and the operator giving the child a single clear instruction at the moment of the needle. Close the loop with honest feedback ("you were really brave, that pinch is all done") and praise for the coping strategy the child used, which is the single most powerful protection against fear at the next needle. [10] [11]
Specific Subtypes & Scenarios
The bundle is adjusted to the child and the procedure in front of you, and the fellowship candidate must show they can match the layers to the subtype rather than apply a single default. [1] [9]
In the neonate and young infant, the priority is sucrose, breastfeeding and containment around a heel lance or venepuncture. Give oral sucrose 24%, 0.1 to 2 mL about two minutes before, with a dummy for non-nutritive sucking; breastfeed if the mother is available; and use swaddled, supported containment rather than a flat hold-down. Prefer Ametop for topical anaesthesia and avoid EMLA under three months. Minimise repeated heel lances by clustering samples and using alternate heels. [3] [12]
In the preschool and school-age child having a vaccination or cannula, preparation and distraction do most of the work alongside a timed topical. Apply EMLA or Ametop at the planned site early, position the child upright on the parent's lap, and run an absorbing tablet distraction or virtual reality; a vibration-and-cold device suits a single needle. The honest, simple explanation and the agreed coping plan turn a feared event into a manageable one. [8] [7]
In the adolescent, the bundle shifts toward the young person's own preferences and toward needle phobia. Offer a topical or subcutaneous lidocaine, a tablet or virtual reality distraction, and a supine position if they faint; a severe needle phobia may need formal psychological desensitisation, applied tension for vasovagal faints, or procedural sedation for a necessary procedure. Engage the adolescent directly and respect their coping choice. [11] [10]
In the child with developmental disability, autism or communication impairment, the bundle is tailored with extra time, a familiar routine and environment, visual supports and a communication strategy the child uses. Avoid unnecessary restraint, use the comfort layers the child will accept, and plan with the family and carers who know the child's signs best; where cooperation cannot be safely achieved, sedation is kinder than a hold-down. [10] [9]
For the laceration repair or dressing change, topical anaesthesia is combined with distraction and comfort positioning and, for the more painful or prolonged repair, escalated to procedural sedation. Topical adrenaline-tetracaine or lidocaine-epinephrine-tetracaine mixtures can anaesthese an open wound directly, and a timed EMLA or Ametop suits the surrounding intact skin; layer distraction and the parent throughout. [6] [1]
For the procedure that exceeds the bundle — a lumbar puncture, an abscess drainage, a fracture manipulation, a complex burn dressing — the comfort layers remain the foundation but are escalated to formal procedural sedation by a trained team with full monitoring. The bundle and sedation are complementary: the child arrives calm, numbed, distracted and held, and sedation adds safety and amnesia on top. [1] [10]
Complications & Pitfalls
The complications of the comfort bundle run from the rare and serious to the common and avoidable, and the discipline is to prevent the serious one and to stop using the common failures as reasons to abandon the bundle. [2] [9]
The serious complication is methaemoglobinaemia from a prilocaine-containing topical (EMLA), concentrated in infants under three months, preterm babies, and children with G6PD deficiency or concurrent oxidant exposure. It presents as cyanosis unresponsive to oxygen with a chocolate-brown blood and a raised methaemoglobin fraction, and is treated by stopping the agent, oxygen, and intravenous methylene blue in the symptomatic child. The prevention is to choose Ametop or an amide in the at-risk group. [2] [5]
The common complications are minor and avoidable. Allergic contact dermatitis to a topical can occur, more often with the ester amethocaine, and a known ester or PABA allergy points to an amide. Transient skin blanching or erythema under a patch is expected and harmless. Under-dosing by under-timing — applying a topical and proceeding within minutes — gives no analgesia at all and is the commonest reason the bundle is wrongly judged to "not work". [5] [6]
A frequently tested misconception is that distraction and comfort are "just" psychology and therefore optional. The Cochrane evidence is clear that non-pharmacological measures, alone and combined with pharmacological ones, reduce procedural pain, and that omitting them is an evidence and ethics failure, not a time-saving choice. The bundle is standard care. [1] [11]
Prognosis & Disposition
The prognosis after a well-managed procedure is excellent: the child experiences the needle as a tolerable, controlled event, the parent's confidence in the team rises, and the next encounter is easier rather than harder. The disposition is driven by how well the bundle is embedded, not by the individual procedure. [9] [10]
For the child whose needle went well, the protection is forward-looking: honest feedback, praise for the coping strategy, and a plan that carries the same layers to the next procedure. A single good experience can interrupt a developing fear, which is why the disposition includes documenting what worked so the next clinician does the same. [11] [10]
For the child whose needle went badly — an under-timed topical, a hold-down, a distressed parent — the prognosis is a strengthened needle fear and a harder next time unless the loop is deliberately broken. The disposition is to acknowledge the experience, debrief with the family, plan a tailored approach with child-life and, where the fear is entrenched, arrange desensitisation or flag the child for a sedation plan at the next necessary procedure. [11] [1]
For the child with a methaemoglobinaemia event, the prognosis with prompt recognition and methylene blue is excellent, and the disposition includes confirming the diagnosis with a methaemoglobin level, avoiding prilocaine in future, and screening for G6PD deficiency where appropriate. [2] [5]
The strongest prognostic lever is a systems-level commitment to making the bundle the default. Units that apply a comfort pathway to every needle — with topical anaesthesia ordered at triage, sucrose stocked, distraction available, and restraint discouraged — see fewer distressed children over time, less needle phobia, and higher rates of procedure completion, which is the real measure of success. [9] [10]
Special Populations
The bundle is adjusted for the child in front of you, and the fellowship candidate must show they can match the layers to the population rather than apply a single default. [1] [10]
In the neonate and young infant, sucrose, breastfeeding and skin-to-skin are the core, with Ametop preferred over EMLA and a dummy and containment added. The neonate's pain is easy to under-recognise and under-treat, and the default is to assume pain and treat it. [3] [12]
In the child with developmental disability, autism or communication impairment, the bundle is built around the child's routine, communication and sensory needs, with extra time, visual supports, and the family's knowledge of the child's signs. Avoidable restraint is a safeguarding concern, and where cooperation cannot be safely achieved, sedation is the kinder and safer path. [10] [9]
In the needle-phobic child and adolescent, the bundle is escalated to a planned coping strategy, applied tension for vasovagal faints, formal desensitisation where the fear is entrenched, and procedural sedation for a necessary procedure the child cannot otherwise tolerate. Engage the young person directly and respect their coping choice. [11] [10]
In the child with complex chronic illness undergoing repeated procedures, the accumulated fear is the enemy, and the bundle is applied consistently at every encounter, with a documented comfort plan that travels with the child, so that each procedure reinforces safety rather than dread. [9] [1]
In the Indigenous, remote or under-resourced setting, the cheap and high-yield layers — sucrose, breastfeeding, honest explanation and comfort positioning — are the equity intervention, applied as a default regardless of staffing or equipment. The principle that comfort is standard care does not depend on resources. [9] [12]
Evidence, Guidelines & Regional Differences
The evidence base for procedural comfort has matured into a coherent, multi-modal message: combine the layers, time the topical, and make comfort the default. The candidate should know the landmark reviews and the regional deltas that follow from them. [1] [11]
The Cochrane review on non-pharmacological management of infant and young child procedural pain (Pillai Riddell and colleagues, 2015, updated 2023) is the backbone of the infant evidence. It found that breastfeeding, sweet solutions and skin-to-skin reduce procedural pain, and that combining non-pharmacological with pharmacological measures works better than either alone; the updated 2023 version refines the picture without changing the core message. [1]
The Cochrane reviews on sucrose for neonatal heel-lance and on topical anaesthesia for needle-related pain in newborns (Yamada 2023; Foster 2017) establish that sucrose is effective for neonatal procedural pain and that topical anaesthetics reduce needle-related pain in newborns, with the choice of agent shaped by onset time and methaemoglobinaemia risk. The breastfeeding meta-analysis (Shi 2024) confirms that breastfeeding or expressed breast milk reduces blood-sampling pain in term neonates. [3] [4]
The HELPinKIDS framework and its update (Shah, Taddio, McMurtry and colleagues, 2015) systematised vaccine-injection pain reduction into a small number of high-yield, evidence-graded interventions — breastfeeding, sweet solutions, topical anaesthetics and distraction — and is the model for the multi-modal bundle examined worldwide. [11] [9]
Non-pharmacological management of infant and young child procedural pain (Cochrane, 2023)
PMID 37314064
Population: Infants and young children undergoing needle-related and other painful procedures
Comparator: No intervention, placebo, water, or standard care
Key finding
Non-pharmacological measures reduced procedural pain; combining them with pharmacological measures worked better than either alone. Breastfeeding and sweet solutions were effective in infants, with the effect attenuating with age.
The systems evidence from Friedrichsdorf and colleagues (2018, 2020) shows that a hospital-wide "ouchless" pathway — topical anaesthesia ordered at triage, sucrose stocked, distraction standard, restraint discouraged — measurably reduces needle pain and needle phobia across a whole institution, and frames comfort as a quality-improvement and patient-safety target, not an individual clinician's kindness. [9] [10]
Where the evidence is weaker or contested: the optimal sucrose concentration and exact volume for older infants, the comparative role of virtual reality against simpler tablet distraction, the long-term effect of the bundle on adult needle phobia, and the balance between restraint and sedation in the uncooperative child with disability. Each is a defensible topic for the viva. [7] [10]
Exam Pearls
The fellowship examiner expects a candidate who knows the agents, the timings, the mechanisms and the contraindications, and who treats comfort as a standard of care layered around every needle. [1] [9]
The single most testable fact is that the answer is always a bundle, never a single agent, because each layer acts on a different limb of the pain response and the Cochrane evidence shows combinations outperform monotherapy. A candidate who names one measure and stops has failed the question. [1] [11]
The agent timings are heavily examined and frequently inverted: EMLA needs at least 60 minutes under occlusion, Ametop 30 to 45 minutes, LMX4 about 30 minutes, and oral sucrose 24% about 2 minutes before. A topical applied and used within minutes gives no analgesia, and sucrose given as the needle goes in (rather than two minutes before) is under-effective. [2] [3]
The contraindication that is always worth marks is methaemoglobinaemia: EMLA is avoided in infants under three months, preterm babies and G6PD deficiency because prilocaine causes methaemoglobinaemia, and Ametop (an ester) is the safer choice in this group — except in known ester or PABA allergy, where an amide such as LMX4 is used. The treatment of symptomatic methaemoglobinaemia is methylene blue 1 to 2 mg per kilogram intravenously. [2] [5]
The sucrose dose trap is dosing it as millilitres per kilogram or in large volumes; the correct dose is 0.1 to 2 mL absolute, maximum about 2 mL, of a 24% solution given two minutes before. The classic distractors the exam rewards for naming: using EMLA in a neonate; applying a topical and proceeding immediately; giving sucrose as mL/kg; relying on distraction alone in a neonate who needs sucrose; and using a forceful hold-down instead of escalating to preparation or sedation. [3] [9]
References
- [1]Pillai Riddell RR, Bucsea O, Shiff I, et al Non-pharmacological management of infant and young child procedural pain Cochrane Database Syst Rev, 2023.PMID 37314064
- [2]Foster JP, Taylor C, Spence K Topical anaesthesia for needle-related pain in newborn infants Cochrane Database Syst Rev, 2017.PMID 28160271
- [3]Yamada J, Bueno M, Santos L, et al Sucrose analgesia for heel-lance procedures in neonates Cochrane Database Syst Rev, 2023.PMID 37655530
- [4]Shi C, Tang J, Li W, et al Comparative Efficacy of Breastfeeding or Feeding of Breast Milk on Blood Sampling Pain Relief in Full-Term Neonates: A Systematic Review and Meta-Analysis Breastfeed Med, 2024.PMID 38386991
- [5]Taddio A, Gurguis MG, Koren G Lidocaine-prilocaine cream versus tetracaine gel for procedural pain in children Ann Pharmacother, 2002.PMID 11918521
- [6]Arendts G, Stevens M, Fry M Topical anaesthesia and intravenous cannulation success in paediatric patients: a randomized double-blind trial Br J Anaesth, 2008.PMID 18292082
- [7]Gao Y, Xu Y, Liu N, et al Effectiveness of virtual reality intervention on reducing the pain, anxiety and fear of needle-related procedures in paediatric patients: A systematic review and meta-analysis J Adv Nurs, 2023.PMID 36330583
- [8]Baxter AL, Cohen LL, McElvery HL, et al An integration of vibration and cold relieves venipuncture pain in a pediatric emergency department Pediatr Emerg Care, 2011.PMID 22134226
- [9]Friedrichsdorf SJ, Eull D, Weidner C, et al A hospital-wide initiative to eliminate or reduce needle pain in children using lean methodology Pain Rep, 2018.PMID 30324169
- [10]Friedrichsdorf SJ, Goubert L Pediatric pain treatment and prevention for hospitalized children Pain Rep, 2020.PMID 32072099
- [11]Shah V, Taddio A, McMurtry CM, et al Pharmacological and Combined Interventions to Reduce Vaccine Injection Pain in Children and Adults: Systematic Review and Meta-Analysis Clin J Pain, 2015.PMID 26201016
- [12]Sutton R, Lemermeyer G Nonpharmacological Interventions to Mitigate Procedural Pain in the NICU: An Integrative Review Adv Neonatal Care, 2024.PMID 38907705