Paeds · investigations-procedures-and-technology
Procedural consent, preparation and child-life support
Also known as Procedural consent in paediatrics · Informed consent and child assent for procedures · Procedural preparation · Child-life specialist support · Needle fear and procedural distress · Comfort positioning and distraction · Family-centred procedural care
Fellowship-level approach to what wraps around every paediatric procedure: valid informed consent and parental permission, the Appelbaum capacity framework, the AAP four-element assent standard and the doctrine of emergency necessity; the structured pre-procedure preparation conversation by developmental age; the evidence-based roles of child-life specialists, distraction, comfort positioning and parental presence; the bedside comfort bundle of topical anaesthesia, oral sucrose as absolute volume up to 2 mL, breastfeeding and non-nutritive sucking; the recognition and stepwise management of procedural distress and needle fear; and the documentation and quality measures that make the practice defensible across ANZ, UK and North American guidelines.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
- Consent, parental responsibility and mature-minor frameworks
- Procedural pain: topical anaesthesia, preparation, distraction and non-pharmacological support
- Safe paediatric procedural sedation
- Shared decision-making and assent in children
- Family-centred and child-rights-based care
- Trauma-informed paediatric care
Overview & Definition
Picture the four-year-old brought to the emergency department for a cannula, clinging to a parent, who has been told only that "you'll feel a little pinch." Within seconds the child is screaming, the parent is apologising, two nurses are holding the arm down, and the first attempt fails. That scene — played thousands of times a day in children's hospitals — is almost entirely preventable, and it is the territory this page owns. The procedure itself (placing the cannula) lives on another page. What lives here is the consent, the preparation, and the comfort that wrap around every procedure, and that decide whether it succeeds or traumatises. [1] [12]
The American Academy of Pediatrics (AAP) frames consent in paediatrics as a layered, two-part act rather than a single signature. A person with authority — usually a parent holding parental responsibility — gives permission for the intervention, while the child gives assent to the extent they are able to. [1] [5] Consent, in the strict legal sense, is reserved for those who hold decision-making capacity for the specific question, including a capable young person assessed as a mature minor. The 1995 AAP statement formalised this distinction between informed consent, parental permission and assent, and the 2016 clinical report updated it to make assent an affirmative, developmentally meaningful act rather than a passive one. [1] [5]
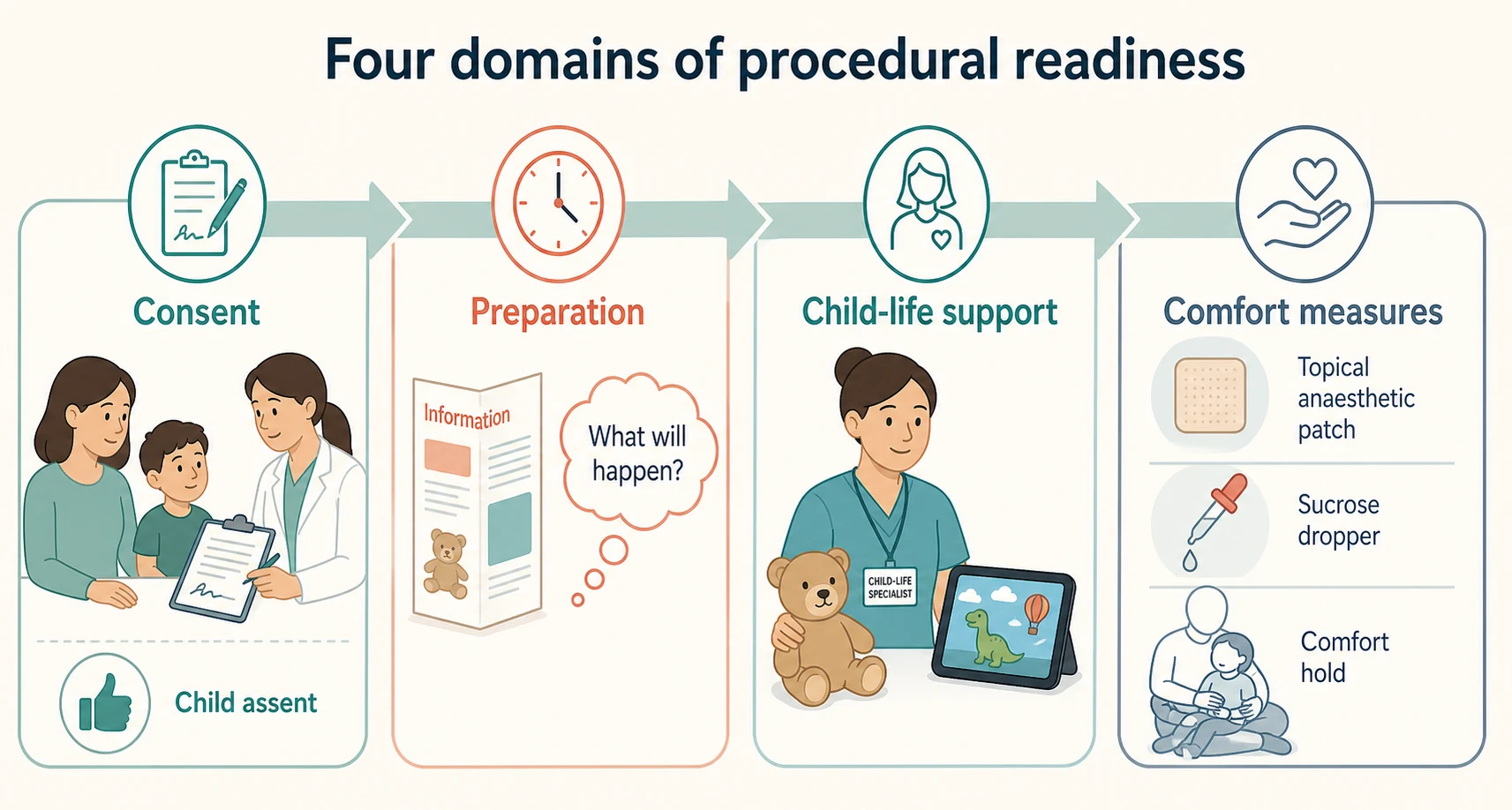
Procedural preparation is the deliberate, timed conversation (and the play, video or rehearsal that accompanies it) that tells a child what they will see, hear and feel, in language matched to their developmental stage, so that they can cope rather than be ambushed. Child-life support is the structured, evidence-informed work of a child-life specialist — a non-medical team member trained in child development, coping and play — who uses medical play, distraction, comfort positioning and coaching to carry a child through a procedure. Comfort measures are the bundled physical and pharmacological acts at the bedside (topical anaesthesia, oral sucrose, breastfeeding, comfort holds, distraction) that reduce the actual nociceptive and emotional load. The three are inseparable in practice, and this page treats them as one system. [7] [11]
Classification
Classify the consent and preparation task by who decides, by how urgent it is, and by what the child can understand, because those three axes determine everything that follows. [1]
By decision-maker, a paediatric procedure falls into one of four pathways. Parental permission is the default for the neonate, infant and young child, where the adult holding parental responsibility authorises the intervention and there is little or no meaningful assent to obtain. Parental permission plus assent is the model for the preschool and school-age child: the parent remains the legal decision-maker, but you seek the child's affirmative agreement and you record and weigh any dissent. Mature-minor consent applies when a young person has sufficient understanding of the specific decision to consent for themselves — a functional, decision-specific assessment, never an automatic birthday. Emergency necessity overrides the sequence entirely: when delay risks death or serious harm and consent cannot be obtained, you treat first and document the basis afterwards. [1] [3] [5]
By urgency, the same procedure — say, intravenous access — moves from an elective, fully prepared pathway to an emergency necessity pathway depending on the child's physiology. The consent and preparation you can do for a cannula in a stable, well child on a ward is not the consent and preparation you can do for the same cannula in a septic, shocked infant; the urgency axis tells you how much of the full preparation you can deploy and what you must defer. [1]
By developmental understanding, the child sits in one of five preparation bands, each with its own cognition, its own fears and its own best modality: the infant (pre-verbal, sensory), the toddler and preschool child (magical thinking, concrete, fear of separation and bodily harm), the school-age child (concrete operational reasoning, a need for honesty and control), and the adolescent (formal operations, autonomy, confidentiality, capacity). The preparation conversation is built differently in each band. [6] [9]
Epidemiology & Risk Factors
Procedural pain and distress in hospitalised children remain substantially undertreated despite decades of evidence and guideline work, and the children most at risk of a difficult or traumatic procedure are also the children who have the most procedures. The risk profile is driven by developmental age, cumulative needle exposure, chronic illness and pre-existing anxiety, and it is amplified by parental anxiety and by staff who default to restraint. [7] [8]
Needle fear is common and tracks across childhood. Roughly two in three children report some needle fear, and in a meaningful minority it reaches phobic intensity that drives vaccination avoidance, healthcare avoidance and procedure refusal into adulthood. The prevalence peaks in late childhood and early adolescence and is higher in children who have had repeated, poorly managed needle procedures, in children with chronic illness, and in children with autism, intellectual disability or sensory processing differences. [7] [11]
Children with medical complexity and technology dependence carry a disproportionate procedural burden — frequent cannulation, blood tests, dressing changes and line care — and are therefore at the highest risk of cumulative procedural trauma. Children in out-of-home care and those with a history of maltreatment arrive with a trauma background that an unexpected, restrained or under-explained procedure can reactivate. Parental anxiety is a direct, measurable predictor of child procedural distress: an anxious, apologetic or hovering parent amplifies the child's fear, while a calm, well-briefed parent who is given a specific, helpful role reduces it. [6] [12]
The single most important epidemiological fact for the fellow to hold is that the procedural trajectory is modifiable. One well-managed procedure measurably improves cooperation and reduces distress at the next one, while each unmanaged painful procedure sensitises the child and the staff. Procedural distress is therefore both a common problem and a preventable harm, and preventing it is the job of this whole page. [7] [9]
Pathophysiology
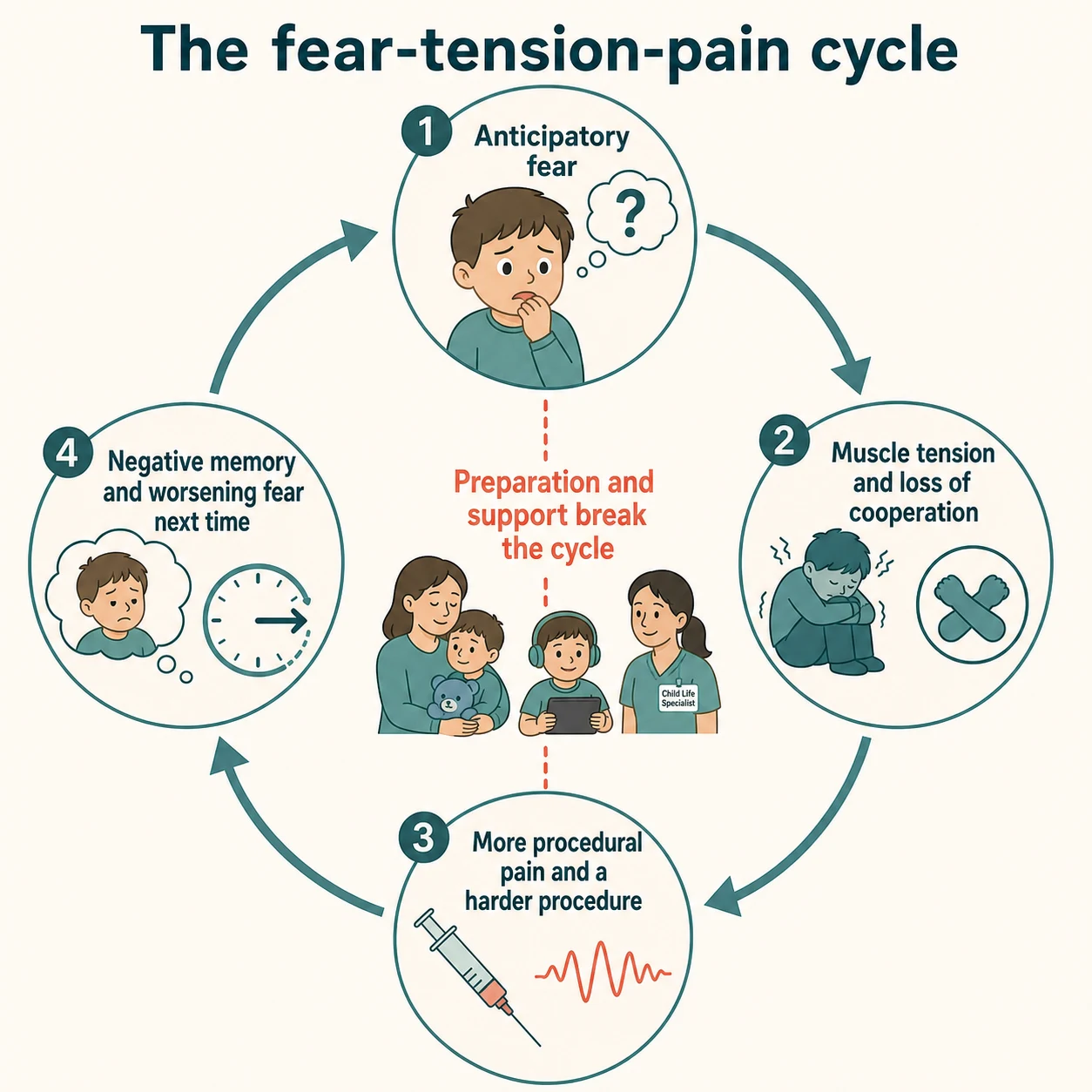
The mechanism that drives procedural distress across repeated procedures is the fear-tension-pain cycle, and understanding it is what turns preparation from a nicety into a treatment. [9]
It starts with anticipatory fear. A child who expects a procedure to hurt allocates attention to the threat, appraises it as dangerous, and their nociceptive system becomes primed — the same noxious stimulus is processed as more painful under conditions of high anxiety and threat appraisal. Fear does not just sit on top of pain; it amplifies it centrally. [9]
Fear then drives muscle tension and loss of cooperation. The frightened child tenses, curls, pulls away or freezes; veins constrict and roll; the procedure becomes technically harder; the operator needs more attempts; and the actual nociceptive load rises. More pain feeds back into more fear. [7]
The cycle closes through memory. A painful, poorly controlled procedure is encoded as a negative emotional memory, and that memory is retrieved at the next procedure as heightened anticipatory fear — so a child who had one bad cannula becomes harder to cannulate next time, regardless of their underlying disease. Memory consolidation is the mechanism by which a single bad procedure becomes a trajectory of procedural trauma and, in some children, a lasting needle phobia. [7] [11]
Developmental cognition shapes where a child enters this cycle. The preschool child holds magical thinking — they may believe the procedure is punishment, or that a cut can never heal, or that the blood will run out — and their fears are therefore concrete, bodily and about separation. The school-age child reasons in concrete operational terms and copes best with honesty, a clear sequence and some control. The adolescent grasps abstract risk and long-term consequences, which both helps their capacity and, in a frightened adolescent, can intensify anticipatory fear. The infant has no cognition of the procedure but a fully intact nociceptive system, which is why procedural pain in infancy is a real, measurable harm and not a non-event. [6] [10]
The comfort measures work because each interrupts the cycle at a different point. Topical anaesthesia removes the nociceptive input at the skin. Oral sucrose activates endogenous opioid and dopaminergic pathways in the infant. Distraction diverts the attention that would otherwise amplify pain centrally. Comfort positioning reduces the tension and the loss of cooperation that make the procedure harder. A calm, briefed parent reduces the threat appraisal. Stacked together, they are more effective than any single intervention — which is exactly what the Taddio additive-effect analysis demonstrated for vaccination pain. [11]
Clinical Presentation
Procedural distress presents differently at each developmental band, and recognising the band-appropriate signal is the first assessment skill. [6]
The infant shows distress behaviourally — a high-pitched cry, facial grimace, brow bulge, body stiffening and arching, and disorganised motor activity — and the validated tool at this age is FLACC or its revised version for cognitively impaired children. The infant cannot tell you what hurts, so you assume pain and treat it; the common error is to under-read infant procedural pain because the child "settled quickly." [10]
The toddler and preschool child present with active resistance, crying, clinging, regression ("I want to go home"), and sometimes freezing or dissociation that can be misread as cooperation. A flat, still, silent child during a procedure is not assenting; they are in a freeze response, and silence is never agreement. [6]
The school-age child may verbalise fear directly, ask detailed questions about what the equipment does, attempt to negotiate ("can you do it on the other arm"), or withdraw and refuse. The Faces Pain Scale and a 0-to-10 numeric scale become usable. The adolescent presents with the full range of adult-typical responses plus the added weight of autonomy and confidentiality — they may refuse outright, may insist on privacy from their parent, or may have a vasovagal faint that is a cardinal feature of needle fear rather than a cardiac event. [7]
- Age-expected fear and distress at a needle or procedure
- Settles with preparation, distraction and a calm parent
- Resolves once the procedure is over and the child is reassured
- Avoidance, refusal, or fainting (vasovagal) at the sight or thought of needles
- Persists across encounters and escalates; drives vaccination and healthcare avoidance
- Needs enhanced preparation, graded exposure, coping skills, and sometimes specialist input
- Silent, still, dissociated child — easily mistaken for cooperation
- History of prior restraint, maltreatment, or repeated unmanaged procedures
- Trauma-informed approach; do not force; reschedule with preparation or sedation
Parental anxiety surfaces at the bedside as excessive reassurance ("it won't hurt at all, be brave"), apologising, hovering, criticising ("you're being a baby"), or sometimes the parent themselves fainting. Each of these amplifies the child's distress and is an indication to pause, reframe the parent's role, and give them a specific, helpful task (a comfort hold, a distraction toy, a calm voice). [7] [12]
The presentation that should make you stop rather than proceed is the child in severe distress or a safety risk, the child in whom you suspect a safeguarding concern, the child whose capacity or dissent you have not properly assessed, and the child who has fainted — these are covered under Management — Resuscitation below. [6] [7]
Differential Diagnosis
The differential of "a child who will not cooperate with a procedure" is short, and every item changes what you do next. [6]
The first distinction is between routine, age-appropriate procedural anxiety and clinically significant needle phobia. Anxiety is universal and settles with the preparation and comfort bundle; phobia is persistent, avoidance-driven, often accompanied by vasovagal fainting, and needs enhanced preparation, graded exposure and sometimes specialist psychological input. Mislabelling a phobia as "non-compliance" abandons a treatable child to escalating healthcare avoidance. [7] [11]
The second distinction is whether the apparent "non-cooperation" is in fact unrecognised pain or an unrecognised sensory difference. A child with autism or sensory processing differences may be refusing because of sensory overwhelm or a predictable-routine disruption, not fear; a child with an unrecognised painful condition may be unable to tolerate an additional procedure on top. [6]
The third distinction is whether the child is lacking capacity, dissenting, or simply frightened. A frightened but capable child can be prepared; a dissenting child's objection must be weighed and recorded; a child who lacks capacity for the decision needs their substitute decision-maker and cannot be over-ridden by persistence. These are not interchangeable, and the assessment of capacity (below) separates them. [1] [3]
The fourth distinction is whether apparent refusal in the adolescent signals an autonomy, confidentiality or safeguarding issue — an undisclosed self-harm concern, a refusal to undress in a parent's presence, or a disclosure that needs a private, capacity-assessed conversation. The adolescent procedural refusal is rarely just about the needle. [1] [6]
Finally, distinguish a vasovagal faint during a needle procedure from a serious cardiac or neurological event. A vasovagal episode in needle fear is preceded by pallor, nausea, diaphoresis and a prodrome, is brief, and recovers quickly with lying flat; a presentation with chest pain, palpitations, exertional syncope, a family history of sudden cardiac death, or a prolonged or atypical collapse changes the differential and warrants cardiac assessment. [7]
Clinical & Bedside Assessment
Before any procedure, run a short, structured assessment that asks four questions: who decides, what does the child understand, what is the child's current state, and is the procedure right now right for this child. This takes two minutes and prevents most of the failures this page exists to prevent. [1]
Who decides is a capacity and authority question. Identify the person with parental responsibility (not simply the adult who brought the child), and assess whether the child can decide for themselves on this specific question. Capacity is assessed with the four Appelbaum domains: the child must understand the relevant information, appreciate the situation and its consequences for themselves, reason about the options, and express a stable choice. Capacity is functional and decision-specific — the same young person may be capable for a low-risk, reversible decision and not for an irreversible one — and it is eroded transiently by pain, fear, hypoxia, hypoglycaemia and delirium, so you treat the reversible cause before concluding a child lacks capacity. [3] [4]
[3] [5]What the child understands is the developmental-assessment question. Place the child in their preparation band, note any autism, intellectual disability or sensory difference, and ask the parent about the child's prior procedural experiences and what helped. This tells you what language, what modality and how much time to use. [6] [9]
What is the child's current state is the distress and pain question. Use an age-appropriate validated tool — FLACC or revised FLACC for infants and cognitively impaired children, the Faces Pain Scale for young children, a 0-to-10 numeric scale for older children and adolescents — and look for the non-verbal signs of freeze or dissociation that a number will miss. A child already in severe distress will not be calmed by a conversation; they need de-escalation and a re-plan. [6] [7]
Is the procedure right, now, for this child is the necessity and timing question. Confirm the indication and the urgency, check that the procedure is truly needed and not a default, confirm who will do it and their competence, and confirm the backup plan. Check fasting status and any pre-procedure results if sedation or a bleeding-risk procedure is contemplated. The honest answer is sometimes "not now" — defer for preparation, for a more experienced operator, or for sedation. [1]
Investigations
There are no laboratory investigations that belong to consent and preparation as a topic; the "investigations" here are the structured assessments and screening tools that select children who need enhanced support, and the documentation that makes the whole encounter defensible. [1]
For the anxious or needle-fearful child, brief, validated screening tools help triage who needs the enhanced pathway. The Children's Fear Scale (a five-face self-report suitable from about age five) and the Children's Anxiety and Pain Scales allow a quick pre-procedure rating; a high score, a history of fainting, or a parent report of avoidance flags the child who should not be booked into a routine slot without child-life input and a coping plan. [7] [11]
For a child with a developmental or cognitive disability, a brief developmental and communication assessment (often already documented in their chart or care plan) informs the consent approach — visual schedules, reduced waiting, sensory adjustments and a familiar carer — and, where capacity is genuinely uncertain, a formal capacity assessment using the Appelbaum domains, sometimes with psychology and ethics input. [3] [6]
The "investigation" that protects every encounter is the consent and preparation record. A defensible record names the procedure, the person who gave consent or assent, the basis on which you are acting (parental permission, the child's own consent as a mature minor, or emergency necessity), the material information disclosed, the capacity findings, whether an interpreter was used, any dissent and how it was weighed, and the time and the clinician. A signature alone is not consent; the documentation of the conversation is. [1] [2]
Finally, treat procedural pain and distress as a quality measure. Audit the proportion of needle procedures performed with topical anaesthesia, with child-life involvement, and with a documented distress score, and track the rate of procedures abandoned or moved to sedation. These metrics tell you whether your unit is managing procedural pain well, and they are increasingly part of accreditation and the patient experience. [7] [12]
Management — Resuscitation
The resuscitation question in this topic is the immediate response to a procedure going wrong or a situation that should not proceed — the child in severe distress or a safety risk, the faint, the emergency without consent, and the parent refusing life-saving care. [1] [7]
Severe distress or a safety risk at the bedside — the child about to strike out, climb off the bed, or be physically held down for a non-emergency procedure — is a stop signal, not a "hold harder" signal. Stop the procedure, move to safety, de-escalate with a calm voice and reduced stimulation, involve the parent in a comfort role, and re-plan: enhanced preparation, a child-life referral, rescheduling with sedation, or a more experienced operator. For a non-emergency procedure, restraint is rarely the right answer, and the distinction between a comfort position (a supported, child-accepting posture that reduces fear and improves access) and restraint (the use of force to overcome active resistance) is both ethical and practical — restraint injures, traumatises and often fails. [6] [7]
A vasovagal faint during a needle procedure is managed by lying the child flat, raising the legs, ensuring the airway is safe, and observing for rapid spontaneous recovery. It is almost always benign, but it is also a marker of clinically significant needle fear that should change the plan for next time. A faint with atypical features — chest pain, palpitations, exertional onset, family history of sudden death, or prolonged collapse — is managed as a potential cardiac event and investigated accordingly. [7]
Emergency treatment without consent is authorised and required by the doctrine of necessity: when a child needs life-saving or serious-harm-preventing treatment and consent cannot be obtained in time, you treat first, document the clinical basis and the attempts to contact a decision-maker, and revisit consent when the child is stable. This applies to the collapsed septic infant needing vascular access and empirical antibiotics, the anaphylactic child needing adrenaline, and the trauma patient needing immediate intervention. The doctrine never licenses treatment beyond what the emergency requires. [1] [5]
Parental refusal of life-saving treatment is the hardest resuscitation-adjacent scenario. The child's welfare overrides parental preference: where a refusal puts a child at risk of death or serious harm, you escalate immediately to a senior clinician, hospital management and (in ANZ) the statutory child-protection authority or (in the UK) the courts, and you provide the urgent treatment under the doctrine of necessity or under emergency statutory authority while the dispute is resolved. Do not simply accept a refusal that endangers the child, and do not delay life-saving care to negotiate. [1]
[6] [7]Management — Definitive & Stepwise
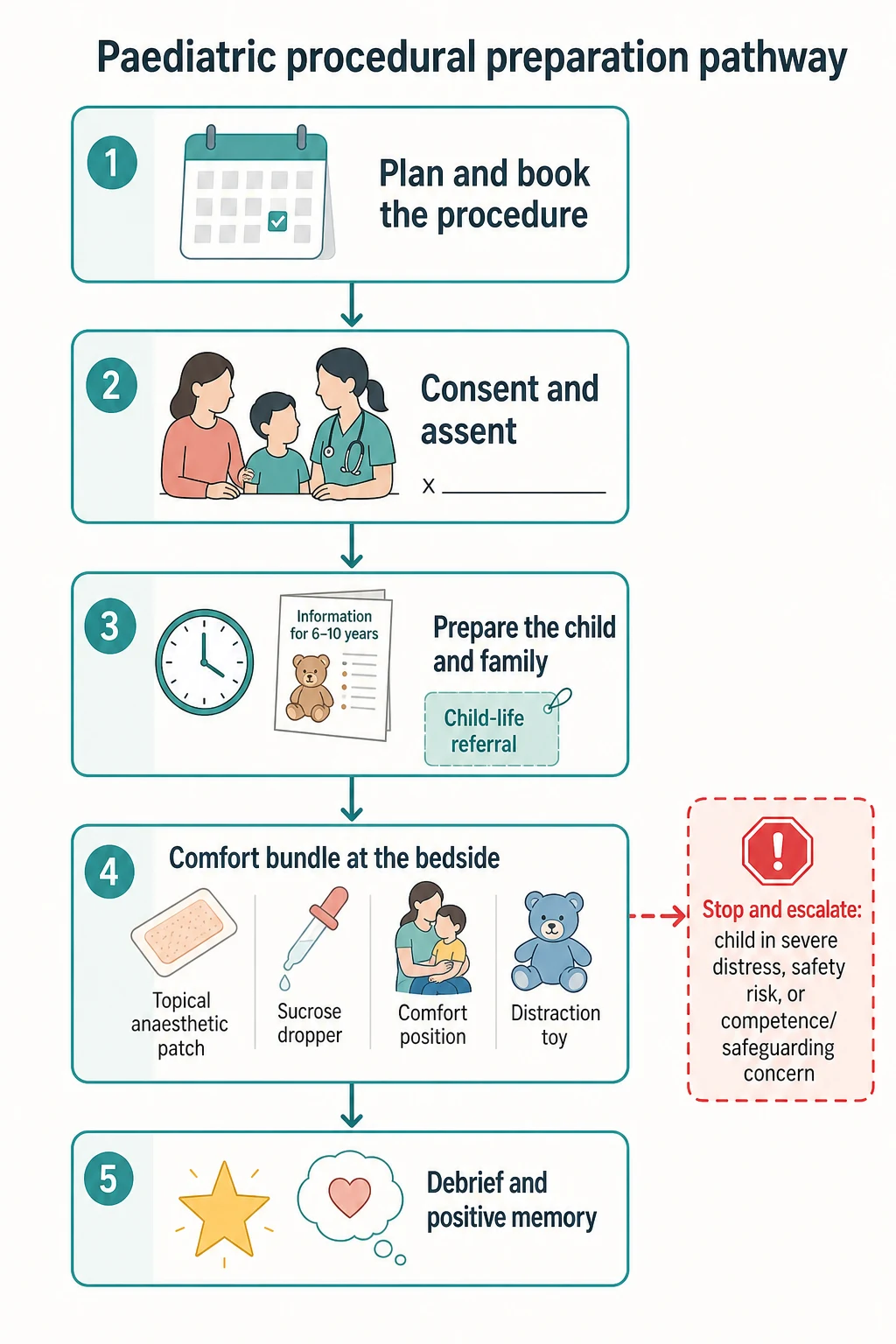
The definitive management is a layered pathway that begins at the moment a procedure is booked and ends with a documented debrief. Build it deliberately, in this order. [1] [11]
The first layer is valid consent and assent. Identify the decision and its urgency, identify the decision-makers, assess capacity for this specific decision, disclose the material information in plain language with teach-back, check understanding and voluntariness, and record the decision and its basis. For the young child, that is parental permission layered with developmentally appropriate assent; for the capable young person, it is their own consent as a mature minor; for the emergency, it is the doctrine of necessity. Use a trained interpreter — never a family member — for any high-stakes consent across a language barrier. [1] [3]
The pre-procedure consent and assent sequence
Identify the decision — the procedure, its indication, its urgency and its risk
Identify the decision-makers — who holds parental responsibility, and can the child decide for this specific question?
Assess capacity and assent potential using the Appelbaum domains and the AAP assent elements
Disclose material information in plain language — what the child will see, hear and feel, the alternatives, and what happens if you do nothing
Check understanding with teach-back and confirm voluntariness — silence and a freeze response are not assent
Obtain and record the decision, the capacity findings, any dissent, the interpreter used, and the basis you are acting on
Plan review points for staged or repeated procedures, and the debrief after
The second layer is preparation. The preparation conversation is timed to the child's developmental band and the procedure's urgency. For an elective procedure, prepare in advance — ideally a day or more for a school-age child, less for a preschool child whose long lead-time breeds more anxiety. For a semi-elective or urgent procedure, prepare at the bedside immediately before, honestly and in concrete terms. The content is constant: what the child will see (the equipment, the tourniquet, the cold spray), what they will hear (the noise, who will be there), what they will feel (the squeeze, the cold, the brief sharpness, the numbness), and what they can do (hold a hand, watch, look away, breathe, squeeze a toy). Honesty is non-negotiable — never say "this won't hurt," because the moment it does, you have lost the child's trust for this procedure and every future one. [6] [9]
- Pre-verbal; preparation is for the parent; the infant's nociceptive system is intact and procedural pain is a real harm
- Comfort holds, oral sucrose, breastfeeding, non-nutritive sucking, swaddling and a calm parent
- Magical thinking and concrete fears; prepare 30 to 60 minutes before, with play and a simple, honest sequence
- Use simple words ('squeeze', 'cold', 'push'), avoid 'this won't hurt', and offer a real choice where one exists
- Concrete reasoning; prepare in advance (a day or more for elective work); give a clear sequence and a coping plan
- Offer genuine control (which arm, count of three, watch or look away) and teach a specific coping strategy
- Abstract reasoning and autonomy; offer a private conversation; assess capacity and confidentiality directly
- Respect the capable young person's own consent or refusal; address needle fear and vasovagal risk explicitly
The third layer is child-life support. A child-life specialist is a non-medical team member trained in child development and coping who uses medical play (letting the child handle a cleaned dummy cannula or a doll before the real procedure), distraction (a bubbles toy, a video, a guided story, a kaleidoscope), coping coaching (a rehearsed breathing or counting strategy), and comfort positioning to carry the child through. The Cochrane review of psychological interventions for needle-related procedural pain and distress found that distraction, combined cognitive-behavioural interventions and hypnosis reduce pain and distress, with the strongest effects when interventions are combined and matched to the child. [7] [8]
The fourth layer is the bedside comfort bundle, and it is where the doses matter. Apply topical anaesthesia (for example, the eutectic mixture of prilocaine and lidocaine, or a 4% lidocaine patch, applied 30 to 60 minutes before for intact skin cannulation) to abolish the nociceptive input at the skin. For the infant, give oral sucrose as an absolute volume — typically 0.1 to 2 mL of 24% to 33% sucrose onto the tongue or a soother two minutes before the procedure, dosed as an absolute volume and not per kilogram, with a maximum of about 2 mL per dose — and offer breastfeeding during the procedure, which the Cochrane review found reduces procedural pain in infants beyond the neonatal period. Add non-nutritive sucking, skin-to-skin contact and a comfort position (chest-to-chest on a parent, side-lying, or hugging a wrapped toy). [10] [11]
The fifth layer is parental presence and role. A calm, well-briefed parent given a specific, helpful task — a comfort hold, a distraction toy, a steady voice — measurably reduces child distress. An anxious, apologetic, critical or hovering parent amplifies it. Brief the parent explicitly on what helps and what harms: a calm, matter-of-fact tone; a single, honest statement; a chosen coping task; and avoiding excessive reassurance, apologising, criticism, or promising it will not hurt. Some adolescents prefer the parent to leave; respect that. [7] [12]
The sixth layer is the escalation ladder for the child who cannot manage a routine pathway. From routine preparation, escalate to enhanced preparation (a child-life referral, a coping plan, a booked slot with reduced waiting), to graded exposure and coping skills for established needle fear (a psychological programme of gradual, supported needle encounters), and, at the top, to pharmacological support or procedural sedation with its own fasting, monitoring and consent pathway. The triggers for escalation are explicit: a documented or parent-reported history of severe distress or fainting, an autistic child needing a predictable low-stimulation environment, repeated failed attempts, or a child who has already deteriorated at this visit. [7]
The seventh and final layer is debrief and documentation. After the procedure, tell the child honestly how it went, praise the specific coping they used (not a vague "you were brave"), and let the parent reinforce the positive memory. Document the procedural distress score, the comfort measures used, whether the procedure succeeded or was abandoned, and what the plan is for the next time. The debrief is not a courtesy; it is the intervention that closes the fear-tension-pain cycle by shaping a positive memory, and it is what turns one good procedure into a better trajectory. [7] [9]
Specific Subtypes & Scenarios
Each developmental and situational band needs its own preparation approach, and the fellow is examined on the differences. [6]
The infant and neonate cannot assent, so the consent is parental permission and the work is comfort and developmental pain relief. Use oral sucrose as an absolute volume (up to 2 mL per dose), breastfeeding during the procedure, non-nutritive sucking, skin-to-skin contact, swaddling where it helps, and a comfort hold. The infant's nociceptive system is mature, and the older myth that infants do not feel or remember procedural pain is false — procedural pain in infancy has measurable physiological and behavioural consequences, and the same comfort bundle that works in the ward works in the neonatal unit. [10]
The preschool child holds magical thinking and fears separation and bodily harm most of all. Prepare 30 to 60 minutes before with play and a simple, honest, concrete sequence; use short words ("squeeze", "cold", "push"); show the equipment on a doll first; avoid "this won't hurt"; and offer a real choice where one genuinely exists (which arm, count of three, watch or look away) — but never a false choice about whether the procedure will happen. [6] [9]
The school-age child reasons concretely and copes best with honesty, a clear sequence and some control. Prepare in advance for elective work, give the child a genuine coping strategy (a rehearsed breathing pattern, a counting task, a chosen video), and let them decide the controllable details. This is the band where child-life coping coaching and distraction have their clearest benefit. [7] [9]
The adolescent needs a private conversation, a direct capacity assessment, an explicit discussion of confidentiality, and respect for their own consent or refusal as a mature minor. Address needle fear and vasovagal risk head-on — a fainting history is common in this band and is manageable with lying positioning, hydration and a calm, slow approach. The adolescent who refuses an urgent procedure needs the same capacity and best-interests analysis as any other decision, never an assumption. [1] [3]
The child with autism, intellectual disability or sensory differences needs a predictable, low-stimulation environment, visual schedules, reduced waiting, a familiar carer present, sensory adjustments (noise-cancelling headphones, dimmed lights, a weighted blanket), and often enhanced preparation or sedation. Capacity is assessed functionally on the same four domains, with adjustment for communication, and the preparation is built around the child's known triggers and coping strategies. [6]
The child in out-of-home care or with a maltreatment history needs a trauma-informed approach — explain everything, offer choice wherever possible, avoid restraint, and recognise that an unexpected procedure can reactivate trauma. The consent authority is the legal guardian (which may be the state, with the carer holding day-to-day authority only), so confirm who can consent, and escalate any safeguarding concern through the usual pathway. [1] [6]
The culturally and linguistically diverse family needs a trained interpreter for consent (never a family member or another child), awareness of cultural and family-decision-making norms, and an offer of a same-gender clinician or chaperone where relevant. For Aboriginal, Torres Strait Islander, Maori and migrant families, a trauma-informed, rights-based approach that includes the family and, where appropriate, an Aboriginal health worker, materially improves both consent quality and the child's experience. [1] [12]
The child facing a series of repeated procedures — the oncology patient, the child with a metabolic or chronic disease, the technology-dependent child — is at the highest risk of cumulative procedural trauma and therefore at the highest priority for a consistent, high-quality preparation pathway. Build a procedural care plan that travels with the child: the coping strategies that work, the staff who do it best, the child-life input, and a debrief after every encounter. One well-managed procedure changes the trajectory for the rest of the treatment. [7] [12]
Complications & Pitfalls
The complications of poor consent and preparation are both immediate and long-lasting, and most are preventable. [1] [7]
The immediate complication is the failed or traumatic procedure: more attempts, more pain, technical failure, a delayed diagnosis or treatment, and a distressed child, parent and staff team. The long-term complications are the fear-tension-pain cycle made chronic — procedural trauma, needle phobia, vaccination and healthcare avoidance into adulthood, and erosion of the child's and family's trust in clinical care. A child who learns that procedures mean being held down and lied to will refuse the next one, and so will the one after. [7] [11]
The consent pitfalls are the classic ethical errors. Treating chronological age as capacity misses the capable 13-year-old and over-rides the incapable 15-year-old. Proceeding on a signature, on silence, or on a leading-question "yes" manufactures false assent — especially in a frightened or freeze-response child. Using a family member as interpreter for high-stakes consent breaches understanding and autonomy. Omitting the assent conversation or the dissent record treats the child as an object. Delaying life-saving care to chase formal consent breaches the doctrine of necessity. [1] [5]
The preparation pitfalls are the timing and content errors. Too much information overwhelms a preschool child; too little ambushes a school-age child; too early breeds anticipatory anxiety; too late leaves no time to cope; and developmentally mismatched language ("just a little pinch", "it won't hurt") sets up betrayal. The script that helps is honest, concrete, short and offers a real coping task; the script that harms is vague, false, apologetic and critical. [6] [9]
The restraint pitfall — using physical force to complete a non-emergency procedure — is both an ethical breach and a clinical failure, and it is the single most damaging thing a team can do to a child's procedural trajectory. The least-restrictive alternative — a comfort position, enhanced preparation, rescheduling, sedation — is almost always available and almost always better. [6] [7]
The parental-behaviour pitfall is the un-briefed parent. Excessive reassurance ("it won't hurt at all"), apologising ("I'm so sorry they're doing this"), criticism ("you're being a baby") and the parent's own fainting all amplify the child's distress; a brief, explicit instruction in the helpful role turns the same parent into the most effective comfort measure available. [7] [12]
The medicolegal pitfall is the undocumented consent. A signature without the conversation, the capacity findings, the material information disclosed, the dissent and the basis on which you are acting is not a defensible consent, and a complaint or a claim will turn on the documentation. [1] [2]
Prognosis & Disposition
The prognosis of a procedural encounter is more modifiable than almost any other outcome in paediatrics, and that modifiability is the central message of this page. A well-managed procedure — valid consent, honest preparation, a child-life-supported comfort bundle, and a documented debrief — predicts a better encounter and a better trajectory; a poorly managed one predicts escalating distress, procedure refusal and, in a meaningful minority, lasting needle phobia and healthcare avoidance. [7] [11]
The long-term trajectory of untreated needle fear is well described: vaccination delay and refusal, healthcare avoidance, and, in the child with a chronic illness, refusal of the very procedures their treatment depends on. The trajectory is interruptible at any point with enhanced preparation, graded exposure, coping skills and, where needed, specialist psychological input, and the earlier the intervention the better the outcome. [7]
Disposition after a difficult procedure is a deliberate decision, not a default. The child who had a single difficult but ultimately well-managed procedure needs a debrief and a documented plan for next time. The child with established needle fear, repeated failed attempts, a fainting history, or a significant developmental or trauma background needs referral to a needle-fear, play-therapy or paediatric-psychology service, and a planned approach for the next procedure that may include sedation. The child in whom a safeguarding concern emerged needs escalation through the usual pathway. [6] [7]
The safety-net after a procedure is the routine one — what to watch for, what analgesia to use, when to return — plus, for the child who had a difficult encounter, a clear, written plan for the next procedure and an offer of enhanced preparation or sedation if needed. [1]
The unit-level prognosis is measured: the proportion of needle procedures performed with topical anaesthesia, with child-life involvement, with a documented distress score, and the rate of procedures abandoned or moved to sedation. A unit that audits and improves these metrics is a unit that has made procedural pain and distress a managed outcome rather than an accepted one. [7] [12]
Special Populations
The consent and preparation approach is tailored, not templated, for each special population, and the tailoring is examined. [6]
For the infant and neonate, consent is parental permission and the work is developmental pain relief — oral sucrose as an absolute volume, breastfeeding, non-nutritive sucking, skin-to-skin and comfort holds. There is no assent to obtain, but there is a fully intact nociceptive system to protect. [10]
For the adolescent and mature minor, consent is a functional capacity assessment for the specific decision, with a private conversation, explicit confidentiality, and respect for the young person's own consent or refusal. The mature-minor threshold is decision-specific and jurisdiction-dependent, and you apply the Appelbaum domains and your local statute and policy. [1] [3]
For the child with autism, intellectual disability or sensory processing differences, the approach is a predictable, low-stimulation environment, visual schedules, reduced waiting, a familiar carer, sensory adjustments, and often enhanced preparation or sedation; capacity is assessed functionally, and the preparation is built around the child's triggers and coping strategies. [6]
For the medically complex and technology-dependent child, who carries the highest procedural burden, the approach is a procedural care plan that travels with the child — the coping strategies, the best staff, the child-life input, and a debrief after every encounter — designed to prevent cumulative trauma over a long treatment. [7] [12]
For the child in out-of-home care, in youth justice, or with a maltreatment history, the approach is trauma-informed — explain everything, offer choice, avoid restraint, recognise trauma reactivation, confirm the legal consent authority, and escalate safeguarding concerns. [1] [6]
For the culturally and linguistically diverse family, and Aboriginal, Torres Strait Islander, Maori and migrant families, the approach uses a trained interpreter for consent, respects cultural and family-decision-making norms, and, where appropriate, includes an Aboriginal health worker. [1] [12]
For the rural and remote child, the child-life specialist may not be physically available, and the approach uses telehealth child-life input, well-trained nursing and medical staff carrying the comfort bundle, and clear referral pathways to a centre with enhanced preparation and sedation capacity. [12]
Evidence, Guidelines & Regional Differences
The evidence base for procedural preparation and comfort is strong on the bundle and weaker on its individual components, and the regional guidelines agree on the principles while differing on the operational thresholds. [7]
The Cochrane review of psychological interventions for needle-related procedural pain and distress (Birnie 2018, updating Uman 2013) is the central evidence document. It found that distraction, combined cognitive-behavioural interventions and hypnosis reduce pain and/or distress in children undergoing needle procedures, with effects strongest when interventions are combined and developmentally matched; the evidence for some individual techniques remains low or very low quality, which is why the bundle, not any single intervention, is the recommendation. [7] [8]
The Cochrane review of breastfeeding for procedural pain in infants beyond the neonatal period (Harrison 2016) found that breastfeeding during a procedure reduces procedural pain in infants up to 12 months compared with no intervention or with maternal holding, supporting breastfeeding as a first-line comfort measure in the breastfed infant. [10]
The Taddio CMAJ analysis of the additive effect of pain interventions during vaccination (2017) showed that combining interventions — feeding, sucrose, distraction and a comfortable position — reduces vaccination pain more than any single component, formalising the bundle as the standard of care for infant vaccination. [11]
The AAP Committee on Bioethics statements (1995 and 2016) define the consent-permission-assent framework that underpins the consent layer, formalising assent as an affirmative, developmentally meaningful act and distinguishing it from consent reserved for those with capacity. [1] [5]
Birnie 2018 — Cochrane review, psychological interventions for needle-related procedural pain
Population: Children and adolescents undergoing needle-related procedures
Key finding
Reduced self-reported pain and distress; strongest effects when interventions are combined and developmentally matched; low or very low certainty for some individual components
In Australia and New Zealand, the RACP and the Royal Children's Hospital Melbourne Comfort Kids guidance frame procedural pain and preparation as a bundled standard of care, with child-life services embedded in tertiary paediatric centres. Mature-minor consent in ANZ follows the common-law capacity test (no fixed age; a functional assessment), informed by the Gillick line of authority. Consent for a child in state care runs through the statutory child-protection authority. [1] [12]
A child-rights framework under the UN Convention on the Rights of the Child frames the child's right to participation in decisions about their care (Article 12) and to protection from violence, including harmful restraint — the basis on which comfort positioning, assent and trauma-informed preparation are rights-based, not merely good practice. The international family-centred care consensus supports this framing. [6] [12]
The controversies are real and examined. Routine sucrose beyond the neonate has weaker evidence but remains widely used and recommended for infant procedural pain up to about 12 months, dosed as an absolute volume. Parental presence is beneficial when the parent is briefed into a helpful role and harmful when the parent is anxious and un-briefed — the variable is the briefing, not the presence. Restraint for non-emergency procedures is increasingly restricted by guidance and policy in favour of comfort positioning and sedation. Mandatory fasting for minor procedures that do not need sedation is a frequent, low-value barrier to timely analgesia and should be challenged. And the evidence base for child-life services as a whole, while supportive, is limited by heterogeneous outcomes and small studies — which is why the recommendation is to deploy the bundle and the child-life specialist together, and to audit the outcomes. [7] [10]
Exam Pearls
PREPARE
The doctrine of necessity authorises and requires emergency treatment when consent cannot be obtained in time and delay risks death or serious harm — treat first, document the basis and the attempts to contact a decision-maker, and revisit consent when the child is stable. [1]
Oral sucrose for procedural pain is dosed as an absolute volume (typically 0.1 to 2 mL of 24% to 33% sucrose, with a maximum of about 2 mL per dose onto the tongue or a soother), not per kilogram — the doses that work are small absolute volumes. [10]
The script that helps versus the script that harms. Helps: honest, concrete, short, a real coping task, a calm matter-of-fact voice. Harms: "this won't hurt," excessive reassurance, apologising, criticism, and promising a reward for no tears. [6] [9]
Restraint is not a comfort position. A comfort position (chest-to-chest on a parent, side-lying, hugging a wrapped toy) is a child-accepting, fear-reducing posture that improves access; restraint is the use of force to overcome active resistance, and it is reserved for the genuine, proportionate, least-restrictive emergency. The distinction is both ethical and practical. [6] [7]
The one-line fellowship answer: valid consent and assent, honest developmentally matched preparation, a child-life-supported bedside comfort bundle, and a documented debrief — layered in that order, for every procedure, because each unmanaged painful procedure sensitises the child for the next. [1] [7] [11]
References
- [1]Katz AL, Webb SA, COMMITTEE ON BIOETHICS Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [2]COMMITTEE ON BIOETHICS Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456514
- [3]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment. N Engl J Med, 1988.PMID 3200278
- [4]Hein IM, De Vries MC, Troost PW, Meynen G Informed consent instead of assent is appropriate in children from the age of twelve: Policy implications of new findings on children's competence to consent to clinical research. BMC Med Ethics, 2015.PMID 26553304
- [5]COMMITTEE ON BIOETHICS, American Academy of Pediatrics Informed consent, parental permission, and assent in pediatric practice. Pediatrics, 1995.PMID 7838658
- [6]Coyne I Children's participation in consultations and decision-making at health service level: a review of the literature. Int J Nurs Stud, 2008.PMID 18706560
- [7]Birnie KA, Noel M, Chambers CT, et al Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst Rev, 2018.PMID 30284240
- [8]Uman LS, Birnie KA, Noel M, Chambers CT, et al Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst Rev, 2013.PMID 24108531
- [9]Jaaniste T, Hayes B, von Baeyer CL Effects of preparatory information and distraction on children's cold-pressor pain outcomes: a randomized controlled trial. Behav Res Ther, 2007.PMID 17727813
- [10]Harrison D, Reszel J, Bueno M, et al Breastfeeding for procedural pain in infants beyond the neonatal period. Cochrane Database Syst Rev, 2016.PMID 27792244
- [11]Taddio A, Riddell RP, Ipp M, et al Relative effectiveness of additive pain interventions during vaccination in infants. CMAJ, 2017.PMID 27956393
- [12]Al-Motlaq MA, Carter B, Neill S, et al Toward developing consensus on family-centred care: An international descriptive study and discussion. J Child Health Care, 2019.PMID 30149735