Paeds · respiratory-sleep-and-airway
Bronchiolitis and viral lower respiratory tract infection
Also known as Acute viral bronchiolitis · RSV bronchiolitis · Viral lower respiratory tract infection · Infant viral wheeze · LRTI in infancy
Fellowship guide to bronchiolitis and viral lower respiratory tract infection: the RSV-driven small-airway obstruction of infancy that gives cough, tachypnoea, wheeze and crackles and difficulty feeding; grading severity by work of breathing, oxygenation and feeding; the differential from viral-induced wheeze, pneumonia, cardiac failure and foreign body; supportive care with feeding, targeted oxygen and high-flow or CPAP rescue while resisting bronchodilators, steroids and antibiotics; nirsevimab and palivizumab prevention; and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the six-week-old brought in on a winter afternoon: two days of a snuffly nose and a wet cough, and now she is breathing fast, her ribs draw in with every breath, there is a fine crackle and a soft wheeze across both lungs, and she has taken only half her feeds since morning. That scene — a young infant with a viral cold that has moved into the chest, breathing hard and feeding poorly — is bronchiolitis, and recognising it lets you settle into calm supportive care rather than a scramble of unhelpful drugs. [1] [2]
Bronchiolitis is an acute viral infection of the bronchioles, the smallest conducting airways, and the name tells you exactly where the trouble sits. The virus inflames the lining of these tiny airways, and the resulting debris, swelling and mucus obstruct airflow at a level where a young infant has very little reserve, which is why a common cold becomes a breathing and feeding problem. [2] [3]
Why this matters at fellowship level is that bronchiolitis is the commonest reason for infants to be admitted to hospital in the first year of life, it is overwhelmingly self-limiting, and it is the classic example of a disease where doing less is doing better. The skill being examined is disciplined supportive care, accurate severity assessment, and the confidence to withhold treatments that feel active but do not help. [1] [3]
Classification
The most useful way to think about a wheezy, coughing infant is to answer two questions at once: is this really bronchiolitis rather than a mimic, and how severe is it right now, because severity drives every decision about oxygen, feeding and admission. [1] [3]
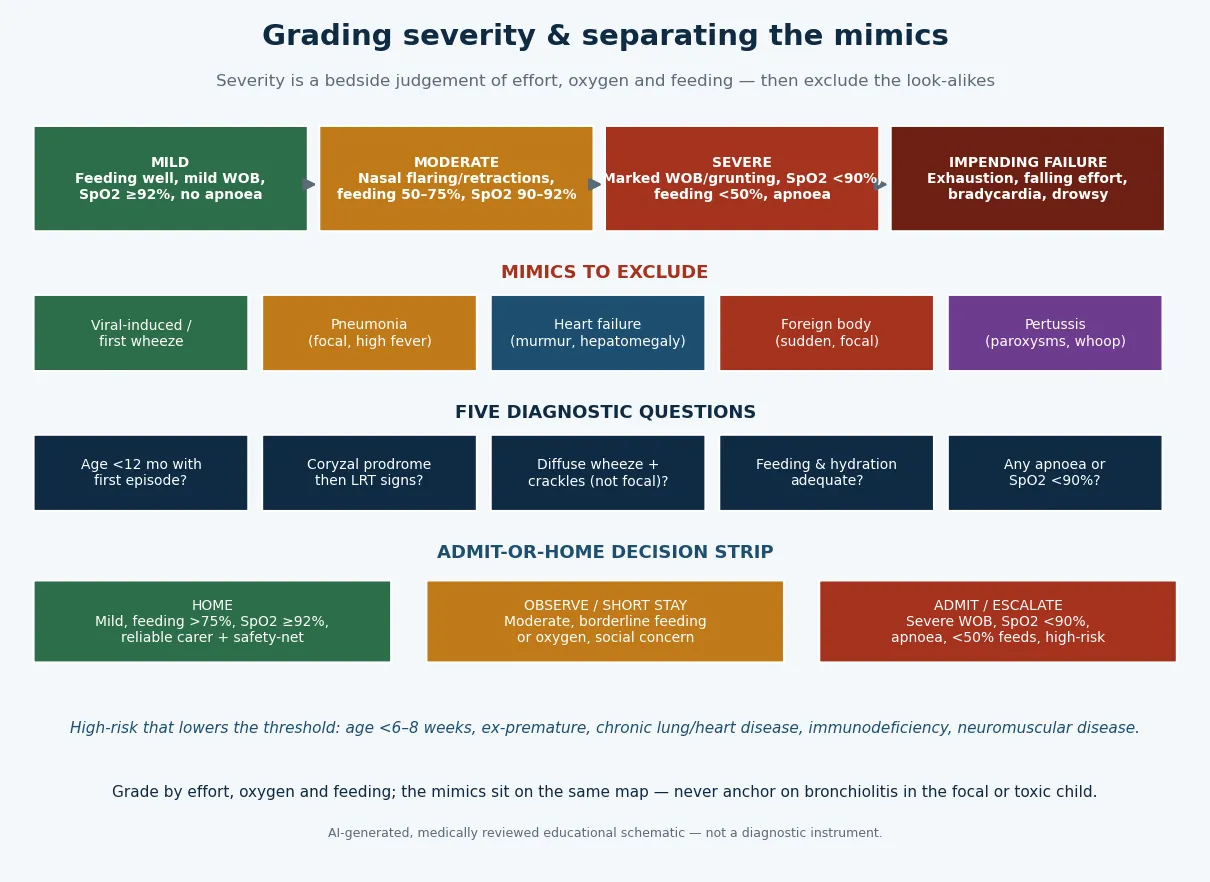
The first axis is diagnostic. The typical patient is a previously well infant under twelve months having a first episode after a coryzal prodrome, with diffuse rather than focal chest signs. A second or later wheezy episode in an older infant or toddler starts to overlap with viral-induced wheeze, and the further a child is from the classic picture, the harder you should look for a mimic. [2] [3]
The second axis is severity, and it is a bedside clinical judgement rather than a score. Mild disease means an infant feeding well with only mild increased effort and normal saturations; moderate disease adds nasal flaring, recession, borderline feeding and saturations around ninety to ninety-two percent; severe disease brings marked effort or grunting, saturations below ninety percent, feeding under half, or apnoea; and impending failure is the exhausted infant whose effort is falling. [1] [3]
The numbers that anchor your viva
Epidemiology & Risk Factors
Bronchiolitis is a disease of the first year of life. It peaks between about three and six months, follows a sharp autumn-to-winter seasonality that tracks circulating respiratory syncytial virus, and is the leading cause of infant hospitalisation across high-income settings, with respiratory syncytial virus responsible for roughly seven in ten cases and other viruses making up the rest. [1] [2]
Most infants have a single self-limiting episode managed at home, but a minority progress to severe disease, and the risk of that progression is concentrated in identifiable groups. The strongest amplifiers are young age, especially under six to eight weeks, and prematurity, because a smaller airway and immature respiratory control leave less reserve when the bronchioles obstruct. [1] [3]
The other high-risk groups reflect reduced cardiorespiratory or immune reserve: chronic lung disease of prematurity, haemodynamically significant congenital heart disease, immunodeficiency, and neuromuscular disease that weakens the cough and the work of breathing. Exposure factors such as household crowding, tobacco smoke and lack of breastfeeding raise the risk of acquiring severe disease as well. [2] [3]
Pathophysiology
The teaching model runs from the virus to the breathless, hypoxic infant, and it turns on one point: the obstruction in bronchiolitis is mechanical, not bronchospastic, which is why the treatments that work in asthma disappoint here. [2] [3]
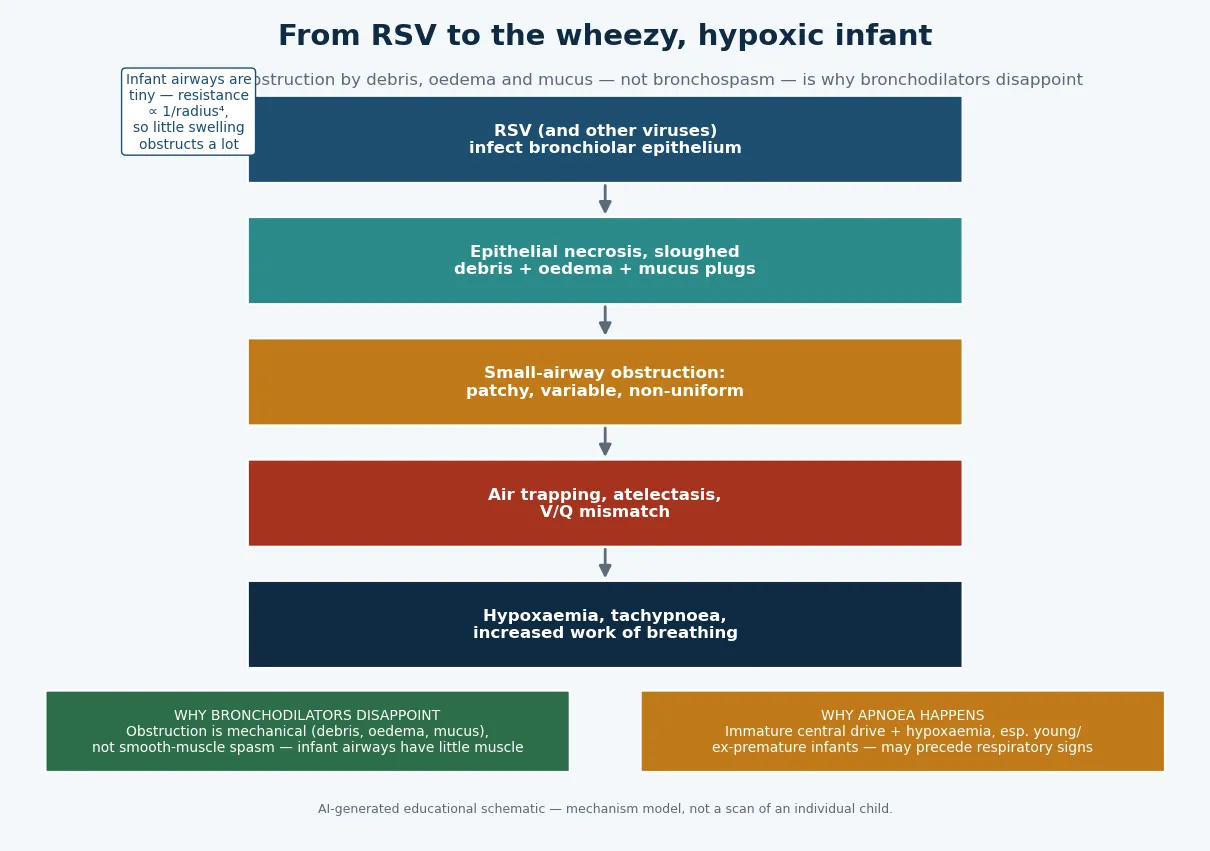
Respiratory syncytial virus, or another respiratory virus, infects and damages the epithelium lining the bronchioles. The dying cells slough into the lumen, the wall becomes oedematous, and mucus secretion increases, so the airway is narrowed by a plug of debris and swelling rather than by tightened muscle. Because these tiny airways have little smooth muscle and the obstruction is patchy, airflow limitation is variable from one bronchiole to the next. [2] [3]
The consequences follow directly from the plumbing. Some airways trap air behind partial obstruction, causing hyperinflation, while others collapse into atelectasis; both disturb the matching of ventilation to perfusion, and this V/Q mismatch is the main reason the infant becomes hypoxaemic. The extra work of moving air past obstruction produces the tachypnoea, recession and grunting you see at the bedside. [3] [2]
A separate strand of the mechanism explains apnoea. Young and ex-premature infants have immature central respiratory control, and the combination of viral illness and hypoxaemia can produce apnoeic pauses that sometimes appear before the chest signs, which is why apnoea is a presenting feature to ask about and observe for, not merely a late complication. [1] [2]
Clinical Presentation
The classic story is a well infant who develops a one-to-three-day coryzal prodrome — runny nose, mild cough, low-grade fever — that then moves into the chest with a worsening cough, fast breathing, audible wheeze and difficulty feeding. Feeding falls before anything else because a breathless infant cannot suck, swallow and breathe at once, so a drop in intake and wet nappies is often the family's first real worry. [1] [2]
The most useful bedside skill is to grade severity from observation before you disturb the infant, because handling can worsen both distress and the reading you get. Watch the respiratory rate and the depth of recession, listen for grunting, note the colour and the conscious level, and ask specifically about feeding and about any pauses in breathing. [1] [3]
| Severity | Bedside picture | Immediate action |
|---|---|---|
| Mild | Feeding well, mild increased work of breathing, saturations at or above 92 percent, no apnoea | Reassure, home with a clear safety-net plan |
| Moderate | Nasal flaring and recession, feeding about half to three-quarters, saturations 90 to 92 percent | Observe, support feeding, oxygen if needed, reassess |
| Severe | Marked recession or grunting, saturations below 90 percent, feeding under half, or apnoea | Oxygen, admit, support feeding, escalate breathing support |
| Impending failure | Exhausted infant, falling respiratory effort, bradycardia, drowsy or unresponsive | Escalate now: high-flow or CPAP, senior and intensive care review |
The trap is the tiring infant. An infant who was working hard and then quietens, with a falling respiratory rate, worsening colour and reduced responsiveness, is not improving — the reduced effort reflects exhaustion, and this is impending respiratory failure. Rising then falling effort in a drowsy infant is an escalation trigger, not a reason for reassurance. [1] [2]
Presentations that sit outside the classic picture should make you reconsider: a high fever with focal crackles pointing to pneumonia, a heart murmur with an enlarged liver suggesting cardiac failure, a sudden choking onset raising a foreign body, or paroxysms of cough with a whoop and post-tussive vomiting suggesting pertussis. Each moves you off simple bronchiolitis toward a diagnosis you must not miss. [2] [3]
Differential Diagnosis
Sort the differential into three groups: the wheeze that is not bronchiolitis (viral-induced wheeze and early asthma), the illnesses that mimic it (pneumonia, cardiac failure, pertussis), and the sudden obstruction of a foreign body. The aim is to confirm bronchiolitis confidently in the typical infant while never anchoring on it when the picture is focal, cardiac or sudden. [2] [3]
Bronchiolitis
the usual answer
- Infant under 12 months, first episode
- Coryzal prodrome then chest signs
- Diffuse wheeze and crackles
- Supportive care only
Viral-induced wheeze
- Older infant or toddler, recurrent
- Wheeze without much crackle
- May respond to a bronchodilator trial
- Consider atopy and asthma pathway
Pneumonia / cardiac
- Focal crackles, high fever, unwell
- Murmur, hepatomegaly, poor feeding, sweating
- Cardiomegaly or focal changes on imaging
- Antibiotics or cardiology as indicated
Foreign body / pertussis
- Sudden choke, focal signs
- Paroxysmal cough, whoop, apnoea
- No coryzal build-up (foreign body)
- Bronchoscopy or macrolide as indicated
Viral-induced wheeze is the commonest source of confusion. An older infant or toddler having a recurrent wheezy episode, often with less crackle and more expiratory wheeze, overlaps with early asthma, and unlike true bronchiolitis it may warrant a monitored bronchodilator trial. The distinction rests on age, on whether this is a first episode, and on the balance of crackles and wheeze. [3] [2]
The dangerous mimics declare themselves by breaking the pattern. Focal crackles with a high fever and a toxic infant suggest bacterial pneumonia; a murmur with hepatomegaly, sweating on feeds and failure to thrive suggests cardiac failure; a sudden choking episode with focal signs suggests an inhaled foreign body; and paroxysmal cough with a whoop, post-tussive vomiting or apnoea suggests pertussis. Recognising these keeps supportive care from becoming a missed diagnosis. [2] [3]
Clinical & Bedside Assessment
Assessment is almost entirely clinical. Take a focused history — the age and gestation at birth, the prodrome and its progression, the pattern of feeding and wet nappies, any apnoea or colour change, immunisation status, and comorbidity such as prematurity or heart disease — and then assess severity while the infant is as settled as possible. [1] [3]
Grade severity by integrating work of breathing, oxygenation and feeding, and use serial assessment rather than a single snapshot to read the trajectory. Respiratory rate, recession, grunting, air entry, colour, conscious level and the ability to feed together tell you far more than any one number, and repeating the assessment after a period of settled observation is what reveals whether an infant is improving or tiring. [1] [3]
Reading the infant, not just the monitor
Severe
Marked effort or grunting, feeding under 50 percent, saturations below 90 percent
Deliberately avoid the things that add nothing and can mislead. There is no need for routine bloods, a routine chest radiograph or routine viral testing in typical bronchiolitis, and over-reliance on a single pulse oximetry reading can drive unnecessary admission or oxygen; interpret saturations alongside effort and feeding, and remember that transient dips during sleep or feeds are common. [1] [8]
Investigations
Bronchiolitis is a clinical diagnosis and needs no routine tests. The default in a typical infant is no bloods, no chest radiograph and no viral swab, because none of them changes management and each carries a cost in distress, radiation or inappropriate treatment. [1] [3]
A chest radiograph is not required to diagnose bronchiolitis and can actively cause harm: the hyperinflation and patchy atelectasis of bronchiolitis are easily misread as consolidation, which drives unnecessary antibiotic prescribing. Reserve imaging for a genuinely atypical or severe picture — a suspected complication, a possible foreign body, an unusual course, or a clinical suspicion of a cardiac or other structural cause. [1] [2]
Viral identification by nasopharyngeal aspirate or PCR does not change the supportive management of an individual infant, but it is useful for cohorting admitted infants and for infection-control decisions during an epidemic. A blood gas has a role only in severe disease or suspected respiratory failure, where it helps judge the need to escalate breathing support. [1] [2]
Management — Resuscitation
For the small number of infants in severe bronchiolitis or impending respiratory failure, the priority is a calm, staged escalation of oxygen and breathing support delivered by the right team, not a scramble for drugs. Minimise handling, keep the infant with the parent where possible, give oxygen to correct hypoxaemia, and summon senior paediatric and intensive care support early. [1] [7]
Correct hypoxaemia with supplemental oxygen, titrated to a target saturation of around ninety to ninety-two percent, because the BIDS trial showed that a target of ninety percent was as safe as ninety-four percent while reducing oxygen use and length of stay. When simple oxygen is not enough, step up to high-flow nasal cannula, which the Franklin trial showed reduces treatment escalation compared with standard oxygen, and then to CPAP, before considering intubation for genuine respiratory failure. [8] [7]
Supportive and preventive agents (not routine ED drugs)
Intubation is rarely needed and is not a routine step even in severe bronchiolitis, because most infants respond to oxygen, high-flow and CPAP that buy time for the illness to turn. When an airway genuinely fails, it is managed in an intensive care setting by the most experienced operator available, with attention to the hyperinflated, obstructed lung and the risk of air leak. [7] [1]
Management — Definitive & Stepwise
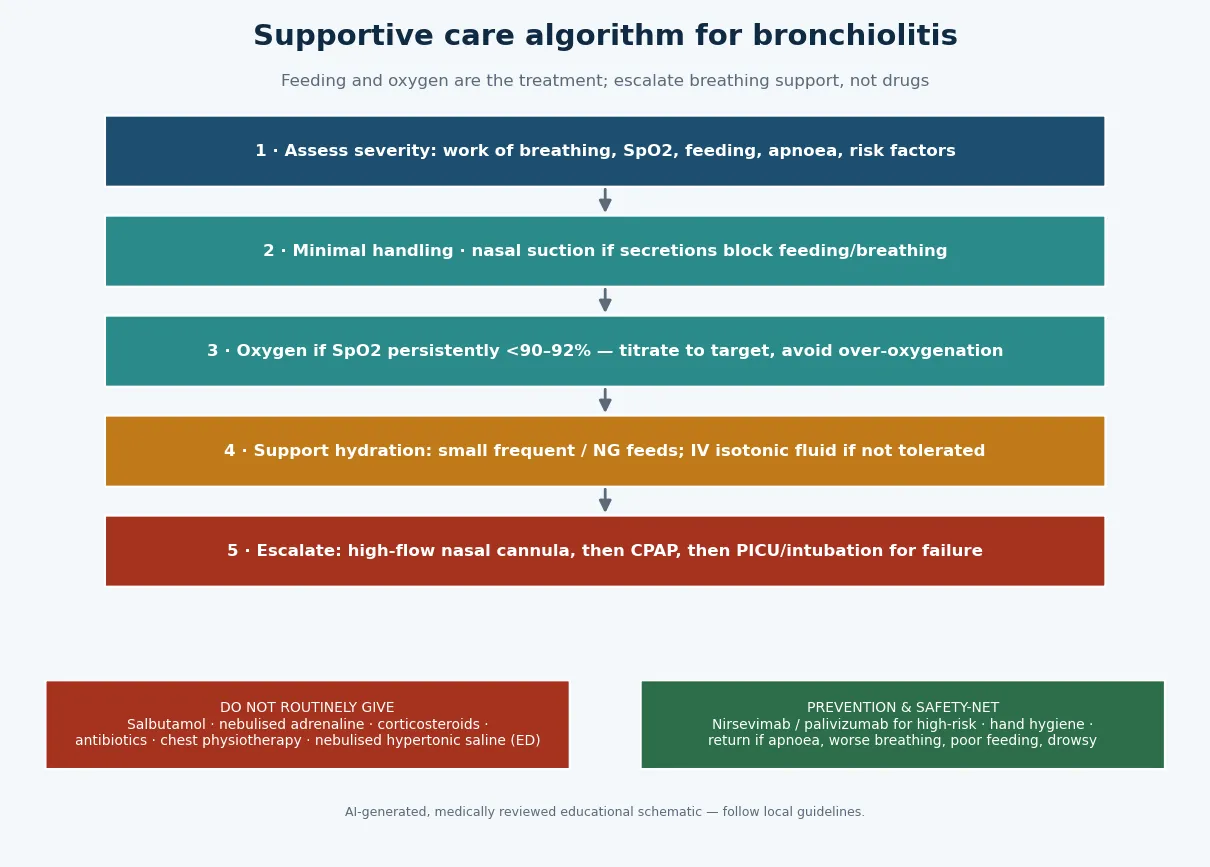
The definitive management of bronchiolitis is deceptively simple and evidence-based: support feeding and hydration, give oxygen only when saturations fall, escalate breathing support when needed, and withhold the drugs that do not work. Doing this well, and confidently not doing the rest, is the whole of good care. [1] [3]
Feeding and hydration are the practical core. An infant feeding more than about half to two-thirds of normal can usually continue oral feeds in small frequent amounts; an infant feeding less, or too breathless to feed safely, needs nasogastric feeding as the first-line support, with isotonic intravenous fluid reserved for those who will not tolerate nasogastric feeds, watching for the dilutional hyponatraemia of inappropriate antidiuretic hormone secretion. [1] [3]
The stepwise pathway
Assess severity by observation: work of breathing, oxygenation, feeding, apnoea and risk factors.
Handle minimally; clear the nose with suction only if secretions block feeding or breathing.
Support feeding: small frequent oral feeds, then nasogastric, then isotonic intravenous fluid.
Give oxygen if saturations are persistently below about 90 to 92 percent, titrated to target.
Escalate breathing support: high-flow nasal cannula, then CPAP, then intensive care for failure.
Dispose by feeding, oxygenation and effort: home with safety-net advice, or admit and observe.
The treatments to withhold are as important as the ones to give, because each is intuitively appealing and each has failed in trials. Salbutamol and nebulised adrenaline do not improve oxygenation, admission or length of stay; corticosteroids do not help acute bronchiolitis and the combination of adrenaline and dexamethasone is not recommended for routine use; antibiotics are unnecessary in a viral illness unless there is a specific bacterial indication; and chest physiotherapy provides no benefit. [5] [4]
Nebulised hypertonic saline deserves a careful answer. The Cochrane review suggested a small possible reduction in length of stay among admitted infants, but the effect is inconsistent and it does not help in the emergency department or shorten the illness, so most guidelines do not recommend it as routine care. Racemic and other nebulised adrenaline strategies were tested directly in the Skjerven trial and did not improve outcomes over saline. [6] [11]
SUPPORT
Specific Subtypes & Scenarios
The young or ex-premature infant with apnoea is the scenario that catches candidates out. Apnoea can be the presenting feature before the chest signs, so a young infant with a viral illness and a reported pause needs admission and monitored observation even if the chest looks unremarkable, because further apnoeas and desaturations may follow. [1] [2]
The infant with chronic lung or congenital heart disease has less reserve and a higher risk of severe disease, so the threshold for admission, oxygen and escalation is lower, and these are exactly the infants for whom RSV prevention with nirsevimab or palivizumab is prioritised. Their bronchiolitis may also last longer and recover more slowly. [1] [9]
Franklin 2018 — N Engl J Med (PMID 29562151)
Randomised trial of high-flow nasal cannula versus standard oxygen in infants with bronchiolitis and hypoxaemia
Key finding
Infants started on high-flow had significantly fewer escalations of care than those on standard oxygen, though intensive care admission and length of stay were similar.
Practice change
High-flow nasal cannula is a rescue for infants failing standard oxygen, not a first-line treatment for every infant — escalate to it rather than starting it routinely.
The remote or telehealth presentation is a common exam scenario: a sick infant a long way from a hospital. The priorities are to gauge severity as best you can, ensure oxygen and feeding support are available, arrange retrieval early for moderate-to-severe disease or apnoea, and give the family explicit return advice, because geography removes the safety net of easy reassessment. [3] [1]
Recurrent wheeze after bronchiolitis is common and worth pre-empting for families. A proportion of infants who have significant bronchiolitis, particularly respiratory syncytial virus disease, go on to have recurrent viral wheeze in the following years, and while this overlaps with the asthma trajectory it does not mean the child has asthma; explain it as a tendency that usually settles with age. [2] [3]
Complications & Pitfalls
Serious complications of bronchiolitis are uncommon because the illness is self-limiting, but they do occur: respiratory failure needing high-flow, CPAP or intubation in a minority, apnoea in young infants, dehydration from poor feeding, and, occasionally, secondary bacterial infection or the dilutional hyponatraemia of inappropriate antidiuretic hormone secretion from over-generous hypotonic fluid. [1] [3]
The dominant pitfalls are ones of over-treatment. The first is reaching for drugs that do not work — salbutamol, adrenaline, steroids, antibiotics and physiotherapy — which add cost, distress and side effects without benefit, and which distract from the supportive care that does help. The discipline of withholding them is a marker of good paediatric practice. [5] [4]
The second pitfall is over-investigation, above all the routine chest radiograph whose misread patchiness drives unnecessary antibiotics, and over-reliance on a single oxygen saturation reading that triggers avoidable admission or oxygen. The third is misreading the tiring infant as improving when falling effort actually signals fatigue and impending failure. Each is avoided by grading the infant serially and interpreting the monitor alongside feeding and effort. [1] [8]
[1]Prognosis & Disposition
The prognosis of bronchiolitis is excellent. The great majority of infants recover fully within one to two weeks, although the cough can linger for several weeks, and even among those admitted, the need for intensive care and intubation is uncommon; the long-term outlook is normal for most, with an increased chance of recurrent viral wheeze in early childhood. [2] [3]
Disposition is decided by feeding, oxygenation and effort rather than by a fixed rule. An infant feeding adequately with normal saturations and only mild effort, whose family can reassess and return, can go home with clear advice; an infant with borderline feeding or oxygen, or with social or geographic barriers to return, warrants observation; and an infant with severe disease, apnoea, or persistently low saturations should be admitted and escalated as needed. [1] [3]
Safety-net advice is part of the treatment and must be concrete: return urgently if there are pauses in breathing or colour change, if breathing becomes harder with marked in-drawing, if the infant feeds less than about half or has fewer wet nappies, if they become pale, floppy or drowsy, or if the family is simply worried. Explain that the illness often worsens around days three to five before it improves. [1] [2]
Special Populations
The ex-premature infant and the infant with chronic lung disease obstruct sooner and recover more slowly, so keep a lower threshold for admission, oxygen and escalation, and prioritise these infants for RSV prevention with nirsevimab or palivizumab before and during the season. [1] [9]
The infant with haemodynamically significant congenital heart disease tolerates the added respiratory load poorly and can decompensate, so involve senior and cardiology teams early, watch fluid balance carefully, and again prioritise prevention. Their bronchiolitis can unmask or worsen cardiac failure, so reassess the cardiovascular picture as well as the respiratory one. [9] [1]
The immunocompromised infant may have prolonged viral shedding and a more severe or protracted course, needs earlier senior involvement and infection-control attention, and may warrant specialist input on antiviral or immunoglobulin options that fall outside routine supportive care. [2] [1]
Indigenous, rural and remote infants face the same illness with a thinner safety net: longer distances to reassessment and retrieval, and in some communities a higher burden of severe respiratory disease. The equity interventions are reliable oxygen and feeding support, early retrieval for moderate-to-severe disease, prioritised RSV prevention, and unambiguous return advice suited to the family's circumstances. [3] [1]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Oxygen and support emphasis | Notes |
|---|---|---|---|
| ANZ | PREDICT Australasian guideline and RCH Melbourne | Supportive care; oxygen when saturations fall; high-flow as rescue | Strong do-not-do list; nasogastric feeding first-line |
| UK | NICE NG9 | Clinical diagnosis; oxygen by saturation thresholds | Explicitly advises against bronchodilators, steroids, antibiotics and hypertonic saline |
| North America | AAP clinical practice guideline | Supportive care; targeted oxygen; no routine drugs | Nirsevimab now central to RSV prevention |
| Low-resource | WHO-aligned approaches | Reliable oxygen and feeding support | Access to oxygen and safe observation is the limiting factor |
The evidence backbone you should be able to name starts with the AAP clinical practice guideline, which crystallised the do-not-do approach, and the Cochrane reviews of bronchodilators (Gadomski) and glucocorticoids (Fernandes), which showed no benefit in acute bronchiolitis. The BIDS trial (Cunningham) established that a ninety percent oxygen target is as safe as ninety-four percent, and the Franklin high-flow trial defined high-flow nasal cannula as a rescue rather than a first-line therapy. [1] [5] [4] [8] [7]
For nebulised therapies, the Cochrane hypertonic saline review (Zhang) found at most a small and inconsistent effect on length of stay, and the Skjerven trial showed that racemic adrenaline and inhalation strategy did not improve outcomes. Prevention has been transformed by monoclonal antibodies: palivizumab (IMpact-RSV) reduced hospitalisation in high-risk infants, and the long-acting nirsevimab (Hammitt) now prevents severe RSV disease across late-preterm and term infants, moving prevention into the general population. [6] [11] [9] [10]
The live areas of nuance are the precise oxygen threshold, the place of high-flow versus CPAP and whether high-flow should ever be first-line, the residual uncertainty over hypertonic saline in admitted infants, and the roll-out and cost-effectiveness of universal nirsevimab — a good example of prevention outpacing the older treatment debates. [7] [10]
Exam Pearls
And when you teach bronchiolitis, teach it as the model of high-value paediatric care — feeding and oxygen, calm observation, clear advice and prevention — while never letting the routine of a common illness dull your alertness to the young infant with apnoea or the atypical picture hiding a mimic. [2] [3]
References
- [1]Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics, 2014.PMID 25349312
- [2]Meissner HC. Viral Bronchiolitis in Children. N Engl J Med, 2016.PMID 26735994
- [3]Florin TA, Plint AC, Zorc JJ. Viral bronchiolitis. Lancet, 2017.PMID 27549684
- [4]Fernandes RM, Bialy LM, Vandermeer B, et al. Glucocorticoids for acute viral bronchiolitis in infants and young children. Cochrane Database Syst Rev, 2013.PMID 23733383
- [5]Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev, 2014.PMID 24937099
- [6]Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulised hypertonic saline solution for acute bronchiolitis in infants. Cochrane Database Syst Rev, 2017.PMID 29265171
- [7]Franklin D, Babl FE, Schlapbach LJ, et al. A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [8]Cunningham S, Rodriguez A, Adams T, et al. Oxygen saturation targets in infants with bronchiolitis (BIDS): a double-blind, randomised, equivalence trial. Lancet, 2015.PMID 26382998
- [9]The IMpact-RSV Study Group. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics, 1998.PMID 9738173
- [10]Hammitt LL, Dagan R, Yuan Y, et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N Engl J Med, 2022.PMID 35235726
- [11]Skjerven HO, Hunderi JO, Brügmann-Pieper SK, et al. Racemic adrenaline and inhalation strategies in acute bronchiolitis. N Engl J Med, 2013.PMID 23758233