Paeds · respiratory-sleep-and-airway
Pleural effusion and empyema
Also known as Parapneumonic effusion · Complicated parapneumonic effusion · Empyema thoracis · Pleural infection · Pyothorax
Fellowship guide to paediatric pleural effusion and empyema: the parapneumonic fluid that turns a child's pneumonia into persistent fever and pleuritic pain; Light's criteria and the exudative, fibrinopurulent and organising stages; ultrasound as the pivotal investigation; antibiotics for all, chest drain with intrapleural fibrinolytics or primary VATS for empyema; the excellent long-term prognosis; and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-year-old admitted three days ago with a lobar pneumonia who should be turning the corner but is not: she is still spiking fevers to 39.5 °C, she is breathing fast, she flinches when she coughs, and the intern notices her breath sounds are now stony-dull at the right base. That failure to improve, not any single dramatic sign, is the classic way a parapneumonic effusion announces itself, and recognising it early is what turns a long, complicated admission into a treatable one. [1] [2]
A pleural effusion is simply an abnormal collection of fluid in the pleural space, the potential space between the visceral pleura covering the lung and the parietal pleura lining the chest wall. In children the overwhelming cause is a parapneumonic effusion — fluid that gathers next to a bacterial pneumonia — and when the fluid becomes infected and thick with pus it is called an empyema. [1] [9]
Why this matters at fellowship level is that empyema is not rare and has been rising: it is a predictable, recognisable complication of a common illness, it responds well to the right treatment, and the marks are earned by spotting the child who is not improving, choosing ultrasound over a plain film, and knowing when antibiotics alone will not be enough. [8] [2]
Classification
The single most useful way to think about a paediatric effusion is by how infected and how organised the fluid has become, because that is what decides whether antibiotics alone will work or whether the child needs a drain. Alongside that, the old physiological split into transudate and exudate still helps you reason about the rare non-infective effusion. [1] [7]
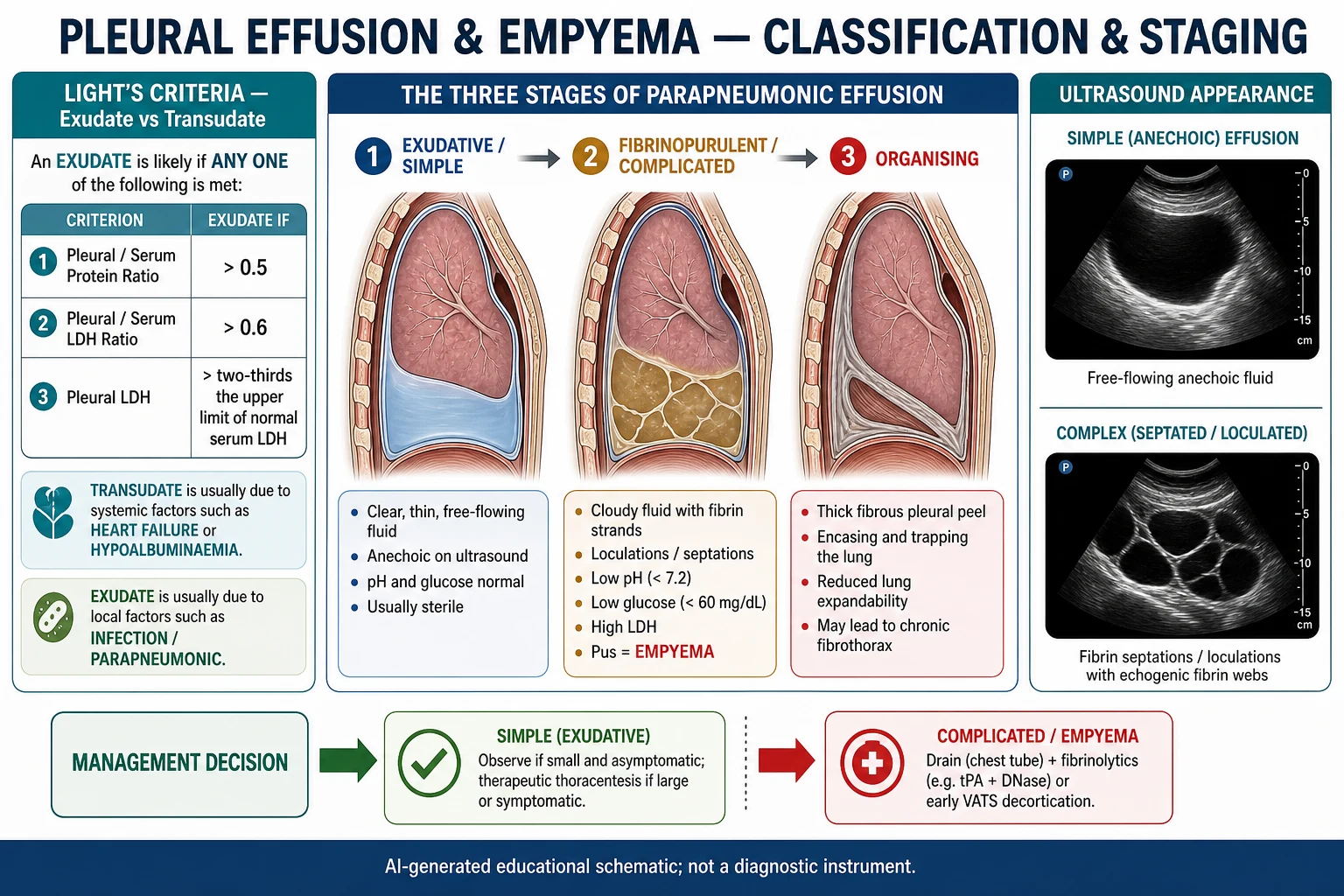
The clinically important classification is the parapneumonic sequence in three stages. The exudative (simple) stage is thin, free-flowing, sterile fluid that follows the inflammation of the underlying pneumonia. The fibrinopurulent (complicated) stage follows bacterial invasion of the fluid, with neutrophils, fibrin strands and loculations, a falling pH and glucose and a rising LDH; frank pus at this point is an empyema. The organising stage sees fibroblasts lay down a thick pleural peel that can trap the lung. [1] [2]
The older transudate-versus-exudate distinction still matters when the picture is not obviously infective. Light's criteria classify an effusion as an exudate if the pleural-to-serum protein ratio is over 0.5, the pleural-to-serum LDH ratio is over 0.6, or the pleural LDH is above two-thirds of the upper limit of normal serum LDH. A transudate points to a systemic cause such as heart failure or hypoalbuminaemia, whereas an exudate points to infection, malignancy or inflammation. [7] [1]
The numbers that anchor your viva
Epidemiology & Risk Factors
Empyema is largely a disease of otherwise healthy young children. It peaks in the preschool years, complicates a small but important fraction of childhood community-acquired pneumonias, and — strikingly — its incidence rose over the 1990s and 2000s in many countries even as invasive pneumococcal disease overall fell after conjugate vaccine introduction, driven partly by non-vaccine pneumococcal serotypes. [8] [9]
The organisms follow a predictable order. Streptococcus pneumoniae is the leading cause, followed by Staphylococcus aureus (including community MRSA in some regions) and Streptococcus pyogenes (group A streptococcus); Haemophilus influenzae is now uncommon where immunisation is high, and anaerobes and Mycobacterium tuberculosis matter in specific settings. Fastidious organisms and prior antibiotics mean pleural fluid cultures are often negative, which is why molecular testing has become useful. [9] [1]
The risk amplifiers are the things that increase exposure to pneumonia or reduce the child's defence and access to care. A preceding viral illness such as influenza or varicella predisposes to bacterial superinfection; immunosuppression and chronic lung disease lower the threshold; and delayed presentation, incomplete immunisation, and distance from timely reassessment all worsen the trajectory of the same infection. [9] [1]
Pathophysiology
The story runs from an inflamed lung to a pocket of pus, and it hinges on the pleura's response to the adjacent infection. In health, a thin film of fluid is constantly produced and reabsorbed across the pleural surfaces; a parapneumonic effusion is a failure of that balance under the pressure of infection. [1] [2]
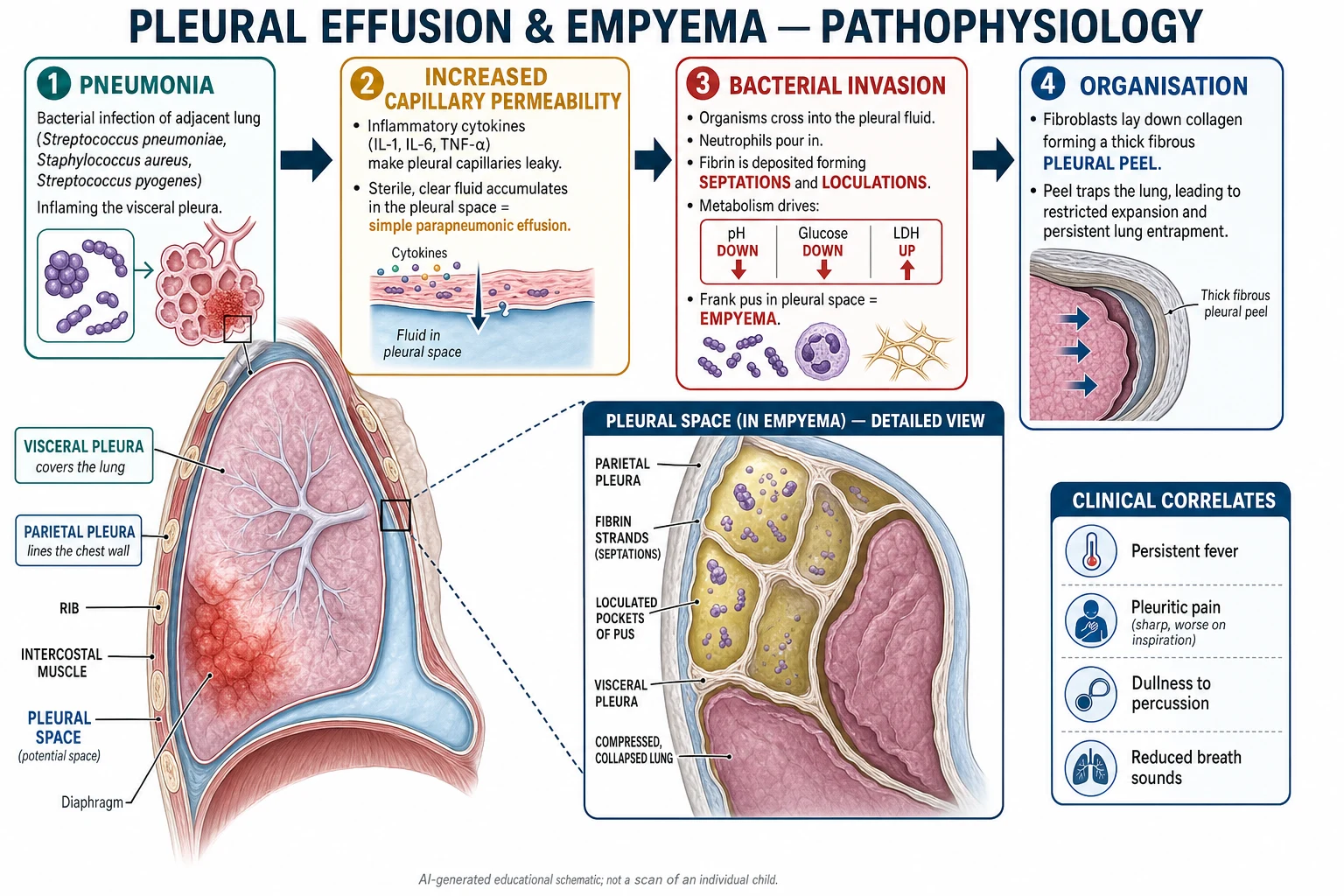
First comes the exudative phase. The pneumonia inflames the visceral pleura, cytokines make the pleural capillaries leaky, and sterile protein-rich fluid accumulates faster than the lymphatics can clear it. If the underlying pneumonia is treated promptly, many of these simple effusions resolve with antibiotics alone. [1] [2]
If bacteria invade the fluid, the fibrinopurulent phase begins. Neutrophils flood in, fibrin is deposited across the pleural surfaces to form septations and loculations, and the metabolic activity of bacteria and white cells consumes glucose and produces acid and lactate dehydrogenase. This is why the biochemical markers of a complicated effusion are a low pH, a low glucose and a high LDH, and why the fluid stops being a single drainable pool and becomes a honeycomb of pockets. [1] [7]
Left unchecked, the organising phase sets in: fibroblasts migrate into the fibrin and lay down a thick, inelastic pleural peel over the lung, restricting its expansion and, in the worst case, trapping it. Recognising which phase the child is in — through the clinical course and the ultrasound — is what matches the treatment to the disease. [1] [2]
Clinical Presentation
The typical child has a pneumonia that is not behaving. After the expected day or two of improvement on antibiotics, the fever persists or returns, the child remains lethargic and off their food, and a new pleuritic chest pain appears — a sharp pain worse on deep breathing or coughing that the child may localise to the chest, the shoulder tip or even the abdomen. [1] [2]
On examination the signs are those of fluid at the lung base: reduced chest expansion on the affected side, stony dullness to percussion, and reduced or absent breath sounds with reduced vocal resonance over the effusion. The child is often tachypnoeic and may lie preferentially on the affected side; an older child may hold themselves stiffly or develop a temporary scoliosis concave toward the effusion to splint the painful side. [1] [2]
| Feature | Uncomplicated pneumonia | Parapneumonic effusion / empyema |
|---|---|---|
| Fever course | Settles within 48–72 h of antibiotics | Persists or returns despite antibiotics |
| Chest pain | Often mild or absent | Prominent pleuritic pain, may refer to abdomen or shoulder |
| Percussion | Dull over consolidation | Stony dull over the fluid |
| Breath sounds | Bronchial over consolidation | Reduced or absent over the effusion |
| Posture | Non-specific | Lies on affected side; may have splinting scoliosis |
The most useful single clue is time. A child whose pneumonia is genuinely failing to improve after two to three days of appropriate antibiotics has a complication until proven otherwise, and a pleural effusion is the commonest one, so persistent fever should trigger an ultrasound rather than a shrug or a longer wait. [1] [10]
Differential Diagnosis
The reasoning has two layers. First, is this dullness at the base actually fluid, or is it dense consolidation, collapse or a raised hemidiaphragm? Second, if it is fluid, is it the usual parapneumonic effusion or one of the less common causes that changes the whole workup? [1] [7]
Parapneumonic / empyema
the usual answer
- Preceding or concurrent pneumonia
- Exudate; low pH, low glucose, high LDH
- Ultrasound: simple or loculated fluid
- Antibiotics plus drainage if complicated
Consolidation / collapse
- Dull but breath sounds bronchial not absent
- No layering fluid on ultrasound
- Air bronchograms on imaging
- Treat the pneumonia; no drain
Non-infective effusion
- Transudate: heart failure, low albumin
- Chylothorax: milky, high triglycerides
- Malignancy: lymphoma, rare in children
- Workup guided by fluid analysis
Tuberculous effusion
- Subacute, weight loss, contact history
- Lymphocytic exudate, high ADA
- Endemic and immunocompromised settings
- Needs anti-tuberculous therapy
Among the fluids, most are parapneumonic, but keep the alternatives in mind when the story does not fit. A transudate (bilateral, no infection, cardiac or renal disease) points away from pleural infection; a chylothorax gives milky fluid rich in triglycerides, often after cardiothoracic surgery or with a lymphatic anomaly; and a malignant effusion from lymphoma or, rarely, another tumour should be considered in the child with systemic features, a mediastinal mass or an atypical course. [7] [1]
Tuberculous pleural effusion deserves its own thought in endemic areas or with a suggestive history: it is typically subacute, with a lymphocyte-predominant exudate and a high adenosine deaminase, and it needs anti-tuberculous treatment rather than a fibrinolytic. Anchoring on a parapneumonic effusion in a child with weight loss, night sweats and a tuberculosis contact is a classic exam trap. [1] [9]
Clinical & Bedside Assessment
Assessment blends a focused history, a careful respiratory examination and an early decision to image. Ask about the pneumonia course and its treatment, the pattern of fever, the chest pain, immunisation status, any preceding viral illness such as influenza or varicella, and any features suggesting tuberculosis or immunocompromise. [1] [9]
The examination is a systematic search for the signs of fluid — expansion, percussion note, breath sounds, vocal resonance — compared side to side, together with the overall assessment of work of breathing, oxygenation and the septic state of the child. Measure the observations, plot the fever, and look specifically for the shift of the trachea and apex beat that warns of a large, tensioning collection. [1] [2]
Reading the size and stage, not just the film
Complicated / empyema
Loculated or purulent fluid, ongoing sepsis
Grade both the size of the collection and its stage (simple versus complicated), because a small simple effusion in a stable child is managed very differently from a large loculated empyema in a septic one. The bedside assessment sets up the pivotal investigation — the ultrasound — rather than replacing it. [1] [2]
Investigations
Two investigations do most of the work: imaging to define the collection, and pleural fluid analysis when fluid is sampled. The chest radiograph is usually the first film and shows a homogeneous opacity with loss of the costophrenic angle or a whole-lung "white-out" with mediastinal shift, but it cannot reliably tell simple fluid from loculated pus and can overcall consolidation as effusion. [1] [2]
Ultrasound is the pivotal test. It confirms that the opacity is fluid, estimates its size, and — crucially — shows whether it is anechoic and free-flowing (simple) or septated and loculated (complicated), which directly guides whether and how to drain. It also marks a safe drainage site. This is why ultrasound, not a CT scan, is the standard next step in a child with a suspected parapneumonic effusion. [1] [2]
When fluid is obtained, send it for Gram stain, culture and pneumococcal PCR, and — on fluid that is not obviously pus — measure the pH, glucose and LDH, applying Light's criteria and remembering that a low pH and low glucose mark a complicated effusion needing drainage. Frank pus is diagnostic of empyema and needs no biochemistry to prove it. Cultures are frequently negative because of prior antibiotics and fastidious organisms, so molecular testing meaningfully raises the diagnostic yield. CT is not routine and is reserved for atypical or non-resolving disease, suspected complications, or a possible underlying lesion. [1] [7]
Management — Resuscitation
For the small number of children who present in extremis — septic, hypoxic, or with a tension effusion — the priorities are the standard sequence applied to a pleural emergency: airway and oxygen, prompt sepsis resuscitation with fluids and intravenous antibiotics, and urgent drainage of a tensioning collection while summoning senior, surgical and intensive care support. [1] [2]
A large effusion causing respiratory compromise or a tension effusion with mediastinal shift needs urgent decompression: a chest drain, guided by ultrasound where time allows, relieves the pressure and improves ventilation. Give supplemental oxygen for hypoxia, provide adequate analgesia so the child can breathe and cough, and correct shock with fluid resuscitation as for any septic child. [1] [2]
Initial drugs in the acutely unwell child
Intubation and ventilation are rarely needed for the effusion itself and, in a tension effusion, drainage is the treatment that relieves the compromise rather than escalating respiratory support. Once the child is resuscitated and the acute pressure relieved, management moves to the stepwise pathway. [1] [2]
Management — Definitive & Stepwise
The definitive management has a clear spine: antibiotics for every child, drainage for the complicated collection, and surgery for the child who does not improve. The art is in matching the aggressiveness of drainage to the stage of the effusion. [1] [2]
Antibiotics for everyone is the foundation. Start intravenous antibiotics that cover the likely organisms — Streptococcus pneumoniae, Staphylococcus aureus and Streptococcus pyogenes, with MRSA cover where it is prevalent — guided by the local guideline, then narrow according to culture and PCR results, and complete a course that is typically extended and stepped down to oral therapy once the child is afebrile and improving. A small, free-flowing, simple effusion in a stable child may resolve on antibiotics alone with careful observation. [1] [2]
The stepwise pathway
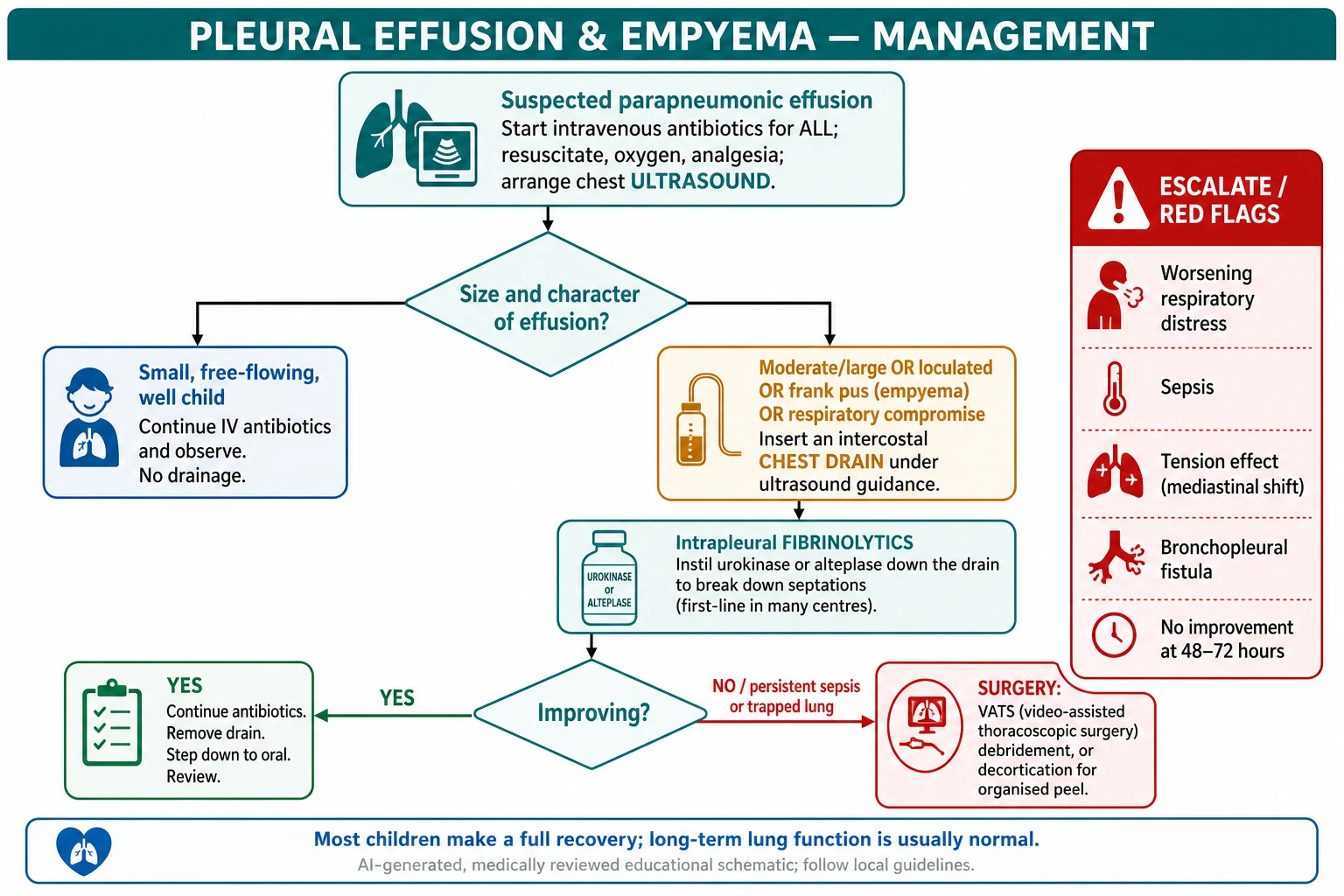
Confirm and stage with ultrasound; start intravenous antibiotics in every child.
Small simple effusion, well child: continue antibiotics and observe, no drainage.
Large, loculated or purulent collection, or respiratory compromise: insert an ultrasound-guided chest drain.
Instil intrapleural fibrinolytics (urokinase) to break down septations in a complicated effusion or empyema.
Reassess at 48–72 hours: if improving, continue and plan drain removal and step-down to oral antibiotics.
If failing — ongoing sepsis, undrained loculation or a trapped lung: proceed to VATS, or decortication for an organised peel.
For a complicated effusion or empyema, the two effective drainage strategies are a chest drain plus intrapleural fibrinolytics and primary video-assisted thoracoscopic surgery (VATS). Randomised trials and a Cochrane review show that both achieve good outcomes; fibrinolytics via a small drain are less invasive and are first-line in many centres, while VATS breaks down loculations directly and is favoured where it is readily available or where fibrinolysis fails. The decision is driven by local expertise and the stage of disease rather than by a universal rule. [3] [4] [6]
Sonnappa 2006 — Am J Respir Crit Care Med (PMID 16675783)
Randomised controlled trial comparing chest drain with intrapleural urokinase versus primary VATS in children with empyema
Key finding
Both treatments gave similar clinical outcomes and length of stay, but urokinase was substantially less expensive than VATS.
Practice change
A chest drain with intrapleural fibrinolytics is a reasonable, less invasive first-line option; VATS is an equally effective alternative, so choice can follow local expertise.
DRAIN
Specific Subtypes & Scenarios
The child who fails fibrinolysis is a common exam and ward scenario. If, after a chest drain and a course of intrapleural fibrinolytics, the child remains septic, the collection is undrained or the lung is trapped, the next step is surgical — usually VATS to break down loculations and evacuate the pus, escalating to decortication where an organised peel restricts the lung. [3] [5]
Staphylococcal empyema, particularly with community MRSA, tends to be more aggressive, is associated with pneumatoceles and lung necrosis, and may complicate a preceding influenza or varicella infection; it needs appropriate anti-staphylococcal (and, where relevant, anti-MRSA) cover and often a more prolonged course. Suspect it in the toxic child with rapidly progressive disease. [9] [1]
Necrotising pneumonia with effusion blurs the line between a pleural and a parenchymal problem: the child has both an effusion and cavitating lung. It is managed with prolonged antibiotics and drainage of the pleural component, but it warrants caution about overly aggressive surgery on the necrotic lung and generally recovers well with time despite alarming imaging. [2] [1]
The remote or resource-limited presentation turns on access rather than choice: ensuring the child receives intravenous antibiotics and a drain, and arranging retrieval to a centre with ultrasound, fibrinolytics or surgery, is the intervention that changes the outcome. In high-tuberculosis settings, a subacute lymphocytic effusion should prompt evaluation for tuberculous pleuritis rather than a fibrinolytic. [1] [9]
Complications & Pitfalls
Most children with empyema recover fully, but the complications are worth naming. Locally, the effusion can cause a tension effusion, a bronchopleural fistula with a persistent air leak, lung necrosis with pneumatoceles, and, in the organising stage, a trapped lung under a fibrous peel; systemically, the child can become septic with metastatic infection. [1] [2]
The dominant pitfalls are of recognition and timing. The first is failing to suspect an effusion in the child whose pneumonia is not improving — attributing persistent fever to the original pneumonia and waiting rather than imaging. The second is relying on the chest radiograph to distinguish simple from loculated fluid instead of using ultrasound, which leads to the wrong drainage decision. [1] [2]
[1] [11]The third pitfall is inadequate or premature drainage: a drain placed into one loculus that leaves the rest behind, or a drain removed before the child has genuinely turned the corner, so the collection re-accumulates. The fourth is anchoring on a parapneumonic cause and missing tuberculosis, a chylothorax or a malignant effusion when the story does not fit. Each is avoided by staging with ultrasound, sending the fluid for the right tests, and reassessing the child against the clock. [1] [7]
Prognosis & Disposition
The prognosis of paediatric empyema is excellent. Despite a course that can be long and alarming — prolonged fever, a chest drain, sometimes surgery — the great majority of children make a complete recovery, and follow-up studies show that long-term lung function and imaging return to normal in most, which is a genuinely reassuring message for families. [2] [1]
Disposition is driven by the stage and the child's response. A child with a small simple effusion who is improving on antibiotics can often be managed on the ward and stepped down to oral therapy for completion at home; a child with a complicated effusion or empyema needs inpatient drainage and observation until the sepsis settles, the drain is out and they are eating, playing and afebrile. The septic, unstable or post-operative child belongs in a high-dependency or intensive care setting. [1] [2]
Follow-up is to confirm resolution and normal recovery: a review with a chest radiograph after several weeks to check the effusion has cleared, and a lower threshold for investigating an underlying cause — such as an immunodeficiency, an aspirated foreign body or a congenital lung lesion — in the child with recurrent or unusually severe disease. [2] [1]
Special Populations
The immunocompromised child — with malignancy, an immunodeficiency or on immunosuppression — is at higher risk, may present atypically, and broadens the differential to include unusual and opportunistic organisms and fungal infection, so early microbiological input and broader cover are warranted. [9] [1]
The child with an underlying respiratory condition — such as a congenital lung malformation, an aspirated foreign body or chronic aspiration — may develop a pleural infection as a marker of that problem; recurrent or localised effusion should prompt a search for a structural or functional cause once the acute illness has settled. [2] [1]
Indigenous, rural and remote families carry a higher burden of severe respiratory infection with a thinner safety net. The equity interventions are prompt recognition, ensuring intravenous antibiotics and drainage are actually delivered, and timely retrieval to a centre with the imaging and surgical resources the illness needs. [9] [1]
Populations with a high tuberculosis burden change the reasoning: a subacute, lymphocyte-predominant effusion with weight loss or a contact history should be evaluated for tuberculous pleuritis and treated with anti-tuberculous therapy, not managed as a bacterial empyema. [1] [9]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | First-line drainage | Notes |
|---|---|---|---|
| ANZ | RCH Melbourne and BTS-aligned pathways | Chest drain plus intrapleural fibrinolytics | VATS if fibrinolysis fails or is unavailable |
| UK | BTS pleural infection in children (2005); BTS pleural disease (2023) | Chest drain plus intrapleural fibrinolytics | Antibiotics for all; ultrasound to characterise |
| North America | APSA review and institutional protocols | Fibrinolytics or primary VATS | Choice varies by centre and surgical availability |
| Low-resource / high-TB | WHO-aligned approaches | Chest drain; consider tuberculosis | Access to ultrasound, fibrinolytics and surgery is limiting |
The evidence backbone you should be able to name starts with the BTS guideline for the management of pleural infection in children (Balfour-Lynn 2005), which set the modern pathway, and its principles are reinforced in the broader BTS pleural disease guideline (2023). The APSA comprehensive review (Islam 2012) synthesised the surgical and medical evidence for empyema in children. [1] [11] [2]
For the drainage decision, the Thomson 2002 randomised trial showed intrapleural urokinase improved drainage over placebo, the Sonnappa 2006 trial found urokinase and VATS clinically equivalent with urokinase far cheaper, and the St Peter 2009 trial similarly found no advantage of primary thoracoscopy over drainage with fibrinolysis; the Cochrane review (Redden 2017) concluded that surgical and non-surgical approaches give broadly comparable outcomes. The epidemiological story — the rising incidence of empyema and the shift in pneumococcal serotypes — comes from Grijalva 2010 and Byington 2002. [3] [4] [5] [6] [8] [9]
The live areas of nuance are the choice between fibrinolytics and primary VATS (driven more by local expertise and cost than by a decisive outcome difference), the optimal antibiotic agent and duration, and how aggressively to intervene in necrotising pneumonia — an area where masterly inactivity often wins. [6] [10]
Exam Pearls
The move that keeps children safe is the disciplined one: in any child whose pneumonia is not improving, image with ultrasound rather than waiting, give antibiotics to everyone, drain the collection that is loculated or purulent, and escalate to surgery for the child who does not turn the corner. [1] [2]
And when you teach empyema, teach it as a reassuring story wrapped in a demanding course — a common complication with an excellent outcome, where the skill is early recognition, the right investigation and matching the drainage to the stage of the disease. [2] [6]
References
- [1]Balfour-Lynn IM, Abrahamson E, Cohen G, et al. BTS guidelines for the management of pleural infection in children. Thorax, 2005.PMID 15681514
- [2]Islam S, Calkins CM, Goldin AB, et al. The diagnosis and management of empyema in children: a comprehensive review from the APSA Outcomes and Clinical Trials Committee. J Pediatr Surg, 2012.PMID 23164006
- [3]Thomson AH, Hull J, Kumar MR, et al. Randomised trial of intrapleural urokinase in the treatment of childhood empyema. Thorax, 2002.PMID 11923554
- [4]Sonnappa S, Cohen G, Owens CM, et al. Comparison of urokinase and video-assisted thoracoscopic surgery for treatment of childhood empyema. Am J Respir Crit Care Med, 2006.PMID 16675783
- [5]St Peter SD, Tsao K, Spilde TL, et al. Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: a prospective, randomized trial. J Pediatr Surg, 2009.PMID 19159726
- [6]Redden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst Rev, 2017.PMID 28304084
- [7]Light RW, Macgregor MI, Luchsinger PC, et al. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med, 1972.PMID 4642731
- [8]Grijalva CG, Nuorti JP, Zhu Y, et al. Increasing incidence of empyema complicating childhood community-acquired pneumonia in the United States. Clin Infect Dis, 2010.PMID 20166818
- [9]Byington CL, Spencer LY, Johnson TA, et al. An epidemiological investigation of a sustained high rate of pediatric parapneumonic empyema: risk factors and microbiological associations. Clin Infect Dis, 2002.PMID 11797168
- [10]Griffith D, Boal M, Rogers T. Evolution of practice in the management of parapneumonic effusion and empyema in children. J Pediatr Surg, 2018.PMID 28781127
- [11]Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax, 2023.PMID 37553157