Acute Asthma Exacerbation
In the United Kingdom, asthma affects approximately 5.4 million people, leading to roughly 75,000 emergency hospital admissions and 1,400 deaths annually. A critical finding in the National Review of Asthma Deaths...
What matters first
In the United Kingdom, asthma affects approximately 5.4 million people, leading to roughly 75,000 emergency hospital admissions and 1,400 deaths annually. A critical finding in the National Review of Asthma Deaths...
Silent chest (no air movement on auscultation)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Silent chest (no air movement on auscultation)
- Normal or rising PaCO2 (indicates respiratory muscle fatigue)
- SpO2 less than 92% on room air
- Exhaustion, confusion, or altered consciousness
Linked comparisons
Differentials and adjacent topics worth opening next.
- Chronic Asthma Management
- COPD Exacerbation
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acute Asthma Exacerbation (Adult)
1. Clinical Overview
Summary
Acute asthma exacerbation is a potentially life-threatening episode characterized by a progressive increase in symptoms of dyspnoea, cough, wheezing, or chest tightness, associated with a decrease in expiratory airflow. This decrease in airflow can be quantified by measurement of peak expiratory flow (PEF) or forced expiratory volume in one second (FEV1). The condition represents a spectrum ranging from a mild "flare-up" to "near-fatal" asthma requiring mechanical ventilation. [1,2]
In the United Kingdom, asthma affects approximately 5.4 million people, leading to roughly 75,000 emergency hospital admissions and 1,400 deaths annually. A critical finding in the National Review of Asthma Deaths (NRAD) was that nearly 45% of patients died without seeking medical help or before emergency care could be provided, highlighting the importance of rapid recognition and treatment. [3,4]
The modern management of acute asthma is based on the rapid administration of high-flow oxygen, frequent nebulized bronchodilators (β2-agonists and anticholinergics), and early systemic corticosteroids. For cases refractory to first-line treatment, intravenous magnesium sulphate has become a standard of care. The ultimate goal is to reverse airway obstruction and correct hypoxia while identifying patients at high risk of respiratory arrest. [5]
Key Facts
- The "Silent Chest": The most dangerous sign in acute asthma. It indicates that airflow is so restricted that no sound is produced; it is a pre-terminal finding requiring immediate resuscitation.
- Normal PaCO2 is ABNORMAL: During an exacerbation, patients should be hyperventilating (low PaCO2). A "normal" PaCO2 (~5.3 kPa / 40 mmHg) indicates the patient is tiring and is a life-threatening feature. [6]
- Steroid Timing: Systemic steroids (Prednisolone or Hydrocortisone) take 4–6 hours to exert a clinical effect. They must be given immediately upon presentation to prevent the late-phase inflammatory response.
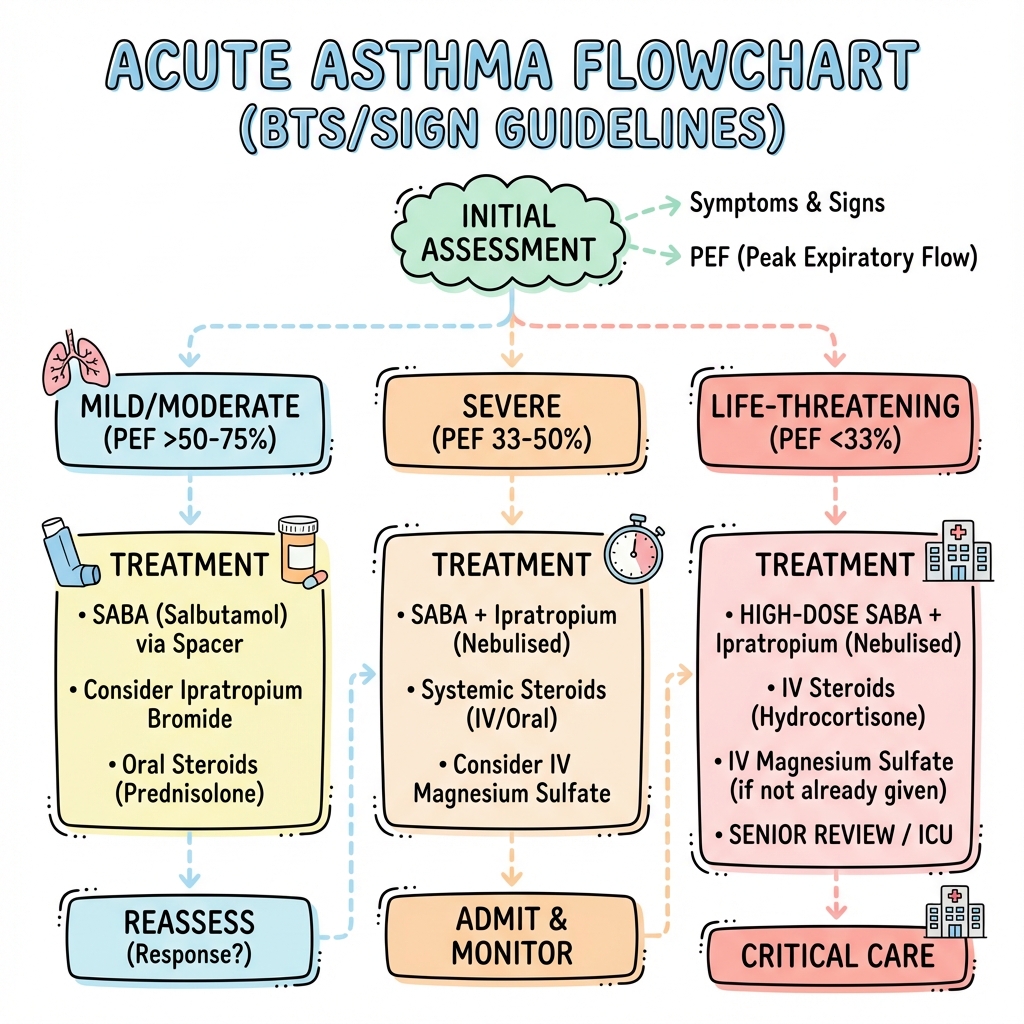
- BTS/SIGN Severity: Severity is classified as Moderate, Severe, Life-threatening, or Near-fatal based on clinical signs and PEF.
- Oxygen Targets: High-flow oxygen is essential initially, but the target SpO2 for stable management is 94–98%. Hypoxia kills far more quickly than hypercapnia in asthma. [7]
Clinical Pearls
The "Sentence" Pearl: If a patient cannot complete a full sentence in one breath, they are by definition in a Severe exacerbation (RR ≥25, HR ≥110, PEF 33-50%).
The "Exhaustion" Pearl: If a patient who was previously agitated and struggling suddenly becomes quiet or "calm," do not be reassured. This often indicates CO2 narcosis or extreme exhaustion—the "quiet before the arrest."
The "Potassium" Pearl: High-dose nebulized Salbutamol drives potassium into cells. Always monitor for hypokalaemia in patients receiving frequent "back-to-back" nebulizers, as this can trigger arrhythmias.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Prevalence: 5–10% of the adult population in Western countries.
- Hospitalization: Asthma accounts for approximately 1 in 20 Emergency Department visits for respiratory distress.
- Seasonality: Peak incidence occurs in the Autumn (September "epidemic" often linked to viral triggers and return to school/work) and late Spring (pollen triggers). [8]
- Gender: In adults, females are more likely to be hospitalized for asthma than males (3:1 ratio), potentially due to hormonal influences on airway inflammation.
Risk Factors for Fatal Asthma
Identifying "at-risk" individuals is vital for preventing mortality. The following factors are associated with a high risk of death: [4,9]
| Category | Risk Factor | Impact |
|---|---|---|
| History | Previous near-fatal asthma | Requires intubation/ICU admission in the past. |
| Utilization | ≥3 ED visits in past year | Marker of poor baseline control and frequent instability. |
| Medication | Overuse of SABA (> 1 canister/month) | Indicates undertreated inflammation and "rescue" dependency. |
| Psychosocial | Poor adherence / Depression | Linked to delayed presentation and failure to follow action plans. |
| Comorbidity | Food allergy (Peanuts/Nuts) | High association with brittle, life-threatening asthma phenotypes. |
3. Pathophysiology
1. The Trigger and Early Phase
Exposure to a trigger (viral infection, allergen, cold air, or NSAIDs in aspirin-sensitive patients) leads to IgE-mediated mast cell degranulation. This releases Histamine, Leukotrienes (LTC4, D4, E4), and Prostaglandins, causing immediate smooth muscle contraction (bronchoconstriction) within minutes. [10]
2. The Late Phase and Inflammation
Starting 4–8 hours after the trigger, a secondary wave of inflammation occurs. Th2 lymphocytes release cytokines (IL-4, IL-5, IL-13) that recruit Eosinophils. These cells release Major Basic Protein and Eosinophil Cationic Protein, which damage the airway epithelium, causing:
- Mucosal Oedema: Increased vascular permeability.
- Mucus Hypersecretion: Thick, tenacious mucus that forms "plugs."
- Airway Remodelling: Long-term structural changes if not controlled. [11]
3. Ventilation-Perfusion (V/Q) Mismatch
Airway narrowing is not uniform. Some areas are more obstructed than others, leading to heterogeneous ventilation. Blood flow to poorly ventilated areas results in a physiological shunt, causing Hypoxaemia. Initially, the patient compensates by hyperventilating, leading to Respiratory Alkalosis (Low PaCO2). [12]
4. Dynamic Hyperinflation
As airflow obstruction worsens, the time required for expiration increases. If the next breath starts before the previous one is fully exhaled, air is trapped (Auto-PEEP). This increases the work of breathing and places the respiratory muscles at a mechanical disadvantage, eventually leading to fatigue.
4. Clinical Presentation
Symptom Evolution
- Prodrome: Increasing use of reliever inhaler, nocturnal wakening, and chest tightness over 2–3 days.
- Acute Phase: Severe breathlessness, inability to talk, and widespread wheezing.
- Exhaustion Phase: If untreated, the wheeze may disappear (silent chest), and the patient becomes drowsy or confused.
Physical Signs by Severity (BTS/SIGN)
| Feature | Moderate | Severe | Life-Threatening |
|---|---|---|---|
| Speech | Sentences | Words/Phrases only | Unable to speak |
| Respiratory Rate | less than 25 bpm | ≥25 bpm | Tiring / Low effort |
| Heart Rate | less than 110 bpm | ≥110 bpm | Bradycardia/Arrhythmia |
| Peak Flow (PEF) | 50-75% | 33-50% | less than 33% |
| SpO2 | ≥92% | less than 92% | less than 92% |
| Other Signs | Wheeze | Accessory muscles | Silent chest / Cyanosis |
5. Investigations
1. Bedside/Primary Assessment
- Peak Expiratory Flow (PEF): Mandatory. Measured as a percentage of the patient's "best" or predicted value.
- Pulse Oximetry: Vital for screening for life-threatening features (SpO2 less than 92%).
- ECG: Usually shows sinus tachycardia. Look for signs of Right Heart Strain (S1Q3T3) or arrhythmias which may indicate severe hypoxia.
2. Arterial Blood Gas (ABG)
Indications: SpO2 less than 92%, life-threatening features, or failing to improve.
- Low PaO2 (less than 8.0 kPa): Hypoxemia is common in severe attacks.
- Low PaCO2 (less than 4.7 kPa): Expected finding; indicates compensation.
- Normal PaCO2 (4.7–6.0 kPa): Life-threatening. Indicates the patient can no longer compensate.
- High PaCO2 (> 6.0 kPa): Near-fatal. Indicates respiratory failure. [6,13]
3. Imaging and Labs
- Chest X-ray: Not routine. Only if suspected pneumothorax, consolidation (pneumonia), or if the patient requires intubation.
- U&Es: High-dose β2-agonists cause Hypokalaemia.
- FBC: May show neutrophilia (due to steroids or infection) or eosinophilia.
6. Management: The Acute Algorithm
Management Flowchart (ASCII)
[ACUTE ASTHMA EXACERBATION]
|
+------------v------------+
| ASSESS SEVERITY (PEF) | (O2, SpO2, RR, HR)
+------------+------------+
|
+--------------------v--------------------+
| IMMEDIATE MEDICAL RX (Simultaneous) |
| 1. Oxygen (Target 94-98%) |
| 2. Salbutamol 5mg Neb (O2 driven) |
| 3. Ipratropium 500mcg Neb |
| 4. Prednisolone 40-50mg PO (or IV HC) |
+--------------------+--------------------+
|
+------------v------------+
| REASSESS @ 15-30 MIN |
+------------+------------+
/ | \
[IMPROVING] [STABLE/POOR] [DETERIORATING]
| | |
+------v------+ +------v------+ +------v------+
| Continue Neb| | IV MAGNESIUM| | CALL ICU/SR |
| q4-6h | | (2g over 20)| | Consider IV |
| Observe 24h | +------+------+ | Aminophylline|
+-------------+ | +--------------+
+------v------+
| RE-EVAL ABG |
+-------------+
1. Pharmacotherapy Detail
- Oxygen: Use the highest concentration available initially (15L Reservoir mask) if life-threatening. Adjust to 94–98% once stable. [7]
- β2-Agonists: Salbutamol 5mg nebulized. In severe cases, use "back-to-back" (continuous) nebulization. Use Oxygen to drive the nebulizer.
- Anticholinergics: Ipratropium Bromide 500mcg every 4–6 hours. Added to Salbutamol in Severe/Life-threatening cases for synergistic effect.
- Corticosteroids: Prednisolone 40–50mg PO daily (minimum 5 days). IV Hydrocortisone (100mg q6h) is only needed if the patient is vomiting or unable to swallow. [14]
2. Escalation (The Magnesium Step)
IV Magnesium Sulphate (2g over 20 mins): Indicated for patients with Severe asthma not responding to initial nebs, or any Life-threatening features. It acts as a potent smooth muscle relaxant. The 3MG trial showed it reduces hospital admission rates in severe cases. [5,15]
3. Critical Care Intervention
Intubation is the last resort due to the high risk of dynamic hyperinflation and tension pneumothorax. Indications for ICU:
- Coma or respiratory arrest.
- Persistently low/falling SpO2 despite maximal therapy.
- Rising PaCO2 or worsening acidosis.
- Exhaustion or silent chest.
7. Complications
- Respiratory Failure (Type 2): Due to muscle fatigue and severe V/Q mismatch.
- Pneumothorax / Pneumomediastinum: Air forced out of the lungs into the pleura or mediastinum due to high pressures.
- Arrhythmias: Triggered by the combination of hypoxia, acidosis, and high-dose β2-agonists.
- Hypokalaemia: A direct side effect of high-dose Salbutamol.
- Atelectasis: Large-scale lung collapse due to mucus plugging. [16]
8. Evidence & Landmark Trials
- 3MG Trial (Lancet 2013): Large RCT showing that while IV magnesium did not significantly improve breathlessness in all comers, it significantly reduced hospital admission rates in patients with severe airflow obstruction (PEF less than 50%). [PMID: 23726145]
- NRAD (National Review of Asthma Deaths 2014): A seminal UK audit that identified major failures in the standard of care, including under-recognition of severity and over-reliance on SABA. [3]
- BTS/SIGN Guidelines (2019): The definitive evidence-based hierarchy for asthma management in the UK, establishing the severity categories used worldwide. [4]
- Cochrane Review (2014): Confirmed that adding Ipratropium to Salbutamol in severe acute asthma reduced hospitalizations and improved lung function. [PMID: 10796464]
9. Single Best Answer (SBA) Questions
Question 1
A 25-year-old female presents with severe breathlessness and wheeze. She can talk in short phrases. RR 28, HR 115, SpO2 93% on air. Her PEF is 45% of predicted. What is the severity of her asthma?
- A) Moderate
- B) Severe
- C) Life-threatening
- D) Near-fatal
- E) Brittle
- Answer: B. Severe asthma is defined by any one of: PEF 33-50%, RR ≥25, HR ≥110, or inability to complete sentences.
Question 2
An ABG is performed on a 30-year-old man with a life-threatening asthma attack. Which of the following results is the most concerning?
- A) pH 7.48, PaCO2 3.2 kPa, PaO2 9.0 kPa
- B) pH 7.40, PaCO2 5.3 kPa, PaO2 8.5 kPa
- C) pH 7.32, PaCO2 6.5 kPa, PaO2 7.0 kPa
- D) pH 7.35, PaCO2 4.0 kPa, PaO2 10.0 kPa
- E) pH 7.50, PaCO2 3.0 kPa, PaO2 11.0 kPa
- Answer: B. A "normal" PaCO2 (5.3 kPa) in the context of severe asthma indicates respiratory muscle fatigue and is a life-threatening sign. (C is near-fatal).
Question 3
What is the mechanism by which Magnesium Sulphate assists in acute asthma?
- A) Reducing eosinophilic inflammation
- B) Potentiating the effect of corticosteroids
- C) Blocking calcium-mediated smooth muscle contraction
- D) Reducing mucus hypersecretion
- E) Increasing the sensitivity of β2-receptors
- Answer: C. Magnesium is a calcium antagonist that causes bronchodilation by relaxing airway smooth muscle.
Question 4
A patient has received three doses of nebulized Salbutamol and Ipratropium. Blood tests show a Potassium of 3.1 mmol/L. What is the most likely cause?
- A) Acute renal failure
- B) Steroid-induced shift
- C) β2-agonist-induced intracellular shift
- D) Excessive urinary loss from IV fluids
- E) Respiratory alkalosis
- Answer: C. Salbutamol stimulates the Na+/K+-ATPase pump, driving potassium into the cells.
Question 5
Which landmark review emphasized that many asthma deaths are preceded by excessive use of short-acting beta-agonists (SABA)?
- A) 3MG Trial
- B) NRAD (National Review of Asthma Deaths)
- C) CODA Trial
- D) E-CLIPS Study
- E) GINA 2023
- Answer: B. NRAD identified that over-prescription and over-reliance on SABA was a major risk factor in fatal cases.
Question 6
A 45-year-old asthmatic presents with life-threatening features. You have given O2 and back-to-back nebs. What is the next most appropriate intravenous medication to administer?
- A) IV Aminophylline
- B) IV Salbutamol
- C) IV Magnesium Sulphate
- D) IV Montelukast
- E) IV Adrenaline
- Answer: C. IV Magnesium is the first-line escalation therapy for severe/life-threatening asthma not responding to nebs.
Question 7
A patient with asthma presents with a silent chest and a heart rate of 50 bpm. What does the bradycardia indicate?
- A) High levels of physical fitness
- B) Vagal response to nebulizers
- C) Impending respiratory and cardiac arrest
- D) Side effect of Magnesium Sulphate
- E) Resolution of the asthma attack
- Answer: C. Bradycardia, silent chest, and exhaustion are late-stage, pre-terminal signs of an asthma attack.
Question 8
How long do systemic corticosteroids typically take to show a significant clinical improvement in acute asthma?
- A) 5–10 minutes
- B) 30 minutes
- C) 1–2 hours
- D) 4–6 hours
- E) 12–24 hours
- Answer: D. Steroids have a delayed onset because they act by modifying gene transcription of inflammatory mediators.
Question 9
Which of the following is a discharge criterion for a patient admitted with acute asthma?
- A) PEF > 50% of predicted
- B) Ability to walk to the toilet without wheezing
- C) PEF > 75% of best or predicted
- D) Completion of 24 hours of IV steroids
- E) Normalization of the chest X-ray
- Answer: C. Patients should be stable on their discharge medication with a PEF > 75% of their best or predicted value.
Question 10
In which of the following scenarios is a Chest X-ray mandatory in acute asthma?
- A) Every patient with a Severe exacerbation
- B) When checking the effectiveness of Salbutamol
- C) Suspected pneumothorax or consolidation
- D) To measure the degree of hyperinflation
- E) To calculate the cardiothoracic ratio
- Answer: C. CXR is only indicated if a complication (pneumothorax/infection) is suspected or if the patient is life-threatening/near-fatal.
12. Airway Dynamics: The Bernoulli Effect and Air Trapping
Why does asthma feel like "suffocating on a full lung"?
A. Dynamic Airway Compression
- The Problem: During an attack, the airway walls are swollen and the muscles are tight (bronchoconstriction).
- The Bernoulli Effect: When you try to breathe out forcefully, the air speed increases through the narrow tube. According to Bernoulli's principle, this higher speed creates a lower internal pressure, which causes the already weakened airway to collapse inward before the air can get out.
- Auto-PEEP: Because air cannot escape, it gets "trapped" in the alveoli. This causes the lungs to over-inflate (hyperinflation), making the next breath even harder to take because the chest is already expanded to its limit.
B. The "Silent Chest" Mechanics
- When air trapping is extreme, there is so little air movement that the characteristic "wheeze" disappears. This is a sign of impending respiratory failure because the energy cost of breathing is exceeding the body's oxygen intake.
13. Molecular Diagnostics: FeNO and Phenotyping
The move toward "Precision Medicine" in the ED.
A. FeNO (Fractional Exhaled Nitric Oxide)
- The Marker: Nitric oxide is a byproduct of Type-2 (T2) inflammation in the airway.
- Clinical Utility: A high FeNO indicates "eosinophilic" asthma, which is highly responsive to inhaled and systemic corticosteroids. If FeNO is low, the asthma may be "neutrophilic" or triggered by other factors, requiring a different management approach.
B. Eosinophilic Phenotyping
- Measuring absolute blood eosinophil counts can help predict which patients are at high risk for future "near-fatal" events and may benefit from early introduction of biologics.
14. Advanced Therapeutics: Magnesium and Biologicals
Beyond Salbutamol and Steroids.
A. The "Magnesium Mystery"
- Mechanism: IV Magnesium Sulphate acts as a calcium-channel blocker in smooth muscle, forcing the airways to dilate.
- The "3MG" Trial Insight: It works best in those with an initial PEF less than 50% of predicted. It "buys time" for the steroids (which take 4-6 hours) to start working on the inflammation.
B. Biologics in Extremis
- While usually for chronic care, the concept of "Interleukin blockers" (like Mepolizumab or Dupilumab) is being studied for severe eosinophilic exacerbations to potentially prevent the rapid return of inflammation after the steroid course ends.
15. Future Trends: Remodeling Prevention
Asthma isn't just "spasams"; it's permanent structural change.
A. Airway Remodeling
- Chronic inflammation leads to the thickening of the basement membrane and the growth of extra smooth muscle. This "remodeling" makes asthma irreversible (COPD-overlap).
- The goal of modern acute care: Rapid suppression of inflammation to prevent this scarring.
B. Bronchial Thermoplasty
- A future potential for patients with frequent severe attacks: Using radiofrequency heat to permanently reduce the amount of smooth muscle in the airway, making severe bronchospasm physically impossible.
16. Patient Explanation
"An asthma attack is like your lungs' breathing tubes suddenly becoming very narrow and swollen, almost like trying to breathe through a thin coffee stirrer that is clogged with glue. The 'blue inhaler' or nebulizer we give you behaves like a key that unlocks those tight muscles, but it only works for a short time. The 'steroid tablets' are the real workers—they go inside the tubes to clear out the 'glue' (swelling). Because steroids take a few hours to start working, we used magnesium to help keep the tubes open in the meantime. You must keep taking your preventer inhaler every day to stop the tubes from becoming scarred and permanently narrowed."
17. Examination Focus: Viva & OSCE Points
The "Silent" Viva
- The ABG Paradox: Explain that a Normal pCO2 in a severe asthma attack is a "Red Flag." It means the patient is tiring out and can no longer blow off CO2. They need HDU/ICU assessment immediately.
- Pulsus Paradoxus: Mention that a drop in systolic BP > 10mmHg during inspiration is a sign of extreme thoracic pressure and severe air trapping.
- Discharge Rules: Know the "75% rule"—patients should not go home unless their Peak Flow is > 75% of their best and stable for 12-24 hours.
18. References
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. 2023. GINA
- British Thoracic Society / SIGN. British Guideline on the Management of Asthma. Thorax. 2019. BTS/SIGN
- Goodacre S, et al. Intravenous or nebulised magnesium sulphate of acute severe asthma: the 3MG randomised controlled trial. Lancet Respir Med. 2013. [PMID: 24429001]
- Royal College of Physicians. Why asthma still kills: The National Review of Asthma Deaths (NRAD). 2014.
- Holgate ST. Pathogenesis of asthma. Clin Exp Allergy. 2008. [PMID: 18452445]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for acute asthma exacerbation?
Seek immediate emergency care if you experience any of the following warning signs: Silent chest (no air movement on auscultation), Normal or rising PaCO2 (indicates respiratory muscle fatigue), SpO2 less than 92% on room air, Exhaustion, confusion, or altered consciousness, Cyanosis (late sign of severe hypoxia), Hypotension or cardiac arrhythmia, PEF less than 33% of predicted or best.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Related Topics
Adjacent pages worth reading next.
- Chronic Asthma Management
- COPD Exacerbation
- Anaphylaxis