EM · Lower gastrointestinal bleed
Lower gastrointestinal bleed
Also known as Lower GI haemorrhage · Acute lower GI bleeding · Haematochezia · Diverticular bleed · Angiodysplasia bleed · Massive lower GI bleed
The lower gastrointestinal bleed — the haemorrhage distal to the ligament of Treitz presenting with haematochezia, dominated by the diverticular bleed (the commonest cause), the inflammatory bowel disease, the colorectal cancer, the angiodysplasia and the haemorrhoids. Risk stratification with the Oakland score (a score of 8 or less predicting safe discharge). Localisation with the CT angiography for the unstable patient and the colonoscopy within 24 hours for the stable. Management with the ABCDE, the fluid resuscitation, the restrictive transfusion to a haemoglobin of 70 g/L, the endoscopic therapy (epinephrine injection and clipping), and the superselective mesenteric angiographic embolisation for the ongoing bleed — always excluding the upper GI bleed with the rapid transit as the mimic. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
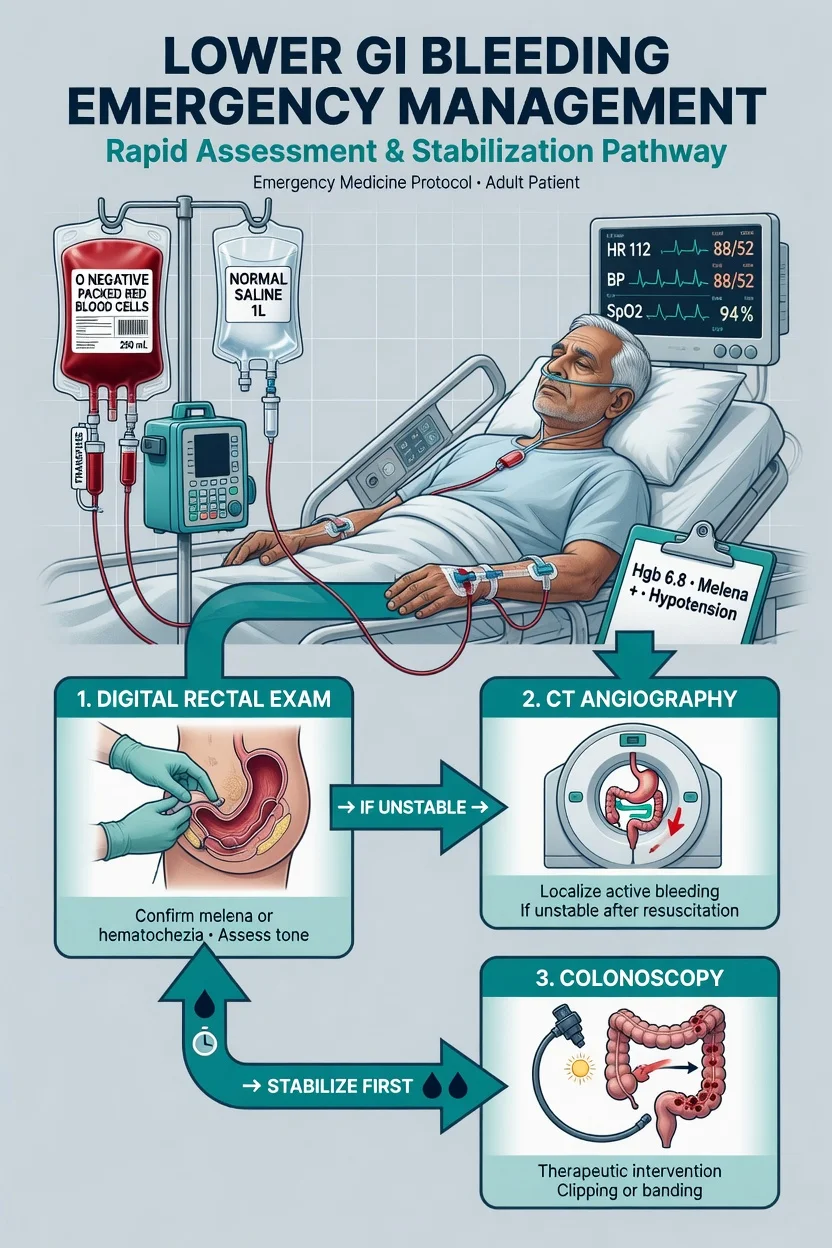
The lower gastrointestinal bleed — any haemorrhage arising distal to the ligament of Treitz — presents as haematochezia, the passage of fresh or maroon blood per rectum, and it is one of the commonest gastrointestinal emergencies of older adults. The Fellowship candidate must hold three patients in mind at once: the well patient with a small anorectal bleed who can be discharged with outpatient colonoscopy; the stable patient who needs colonoscopy within 24 hours; and the unstable, massively bleeding patient who needs CT angiography first followed by superselective mesenteric embolisation. The two errors that fail the station are sending the unstable patient to colonoscopy, and reaching for the upper-GI-bleed drugs (the proton pump inhibitor, the terlipressin, the prophylactic antibiotic) that have no role here. The Oakland score risk-stratifies the stable patient at the bedside, and the restrictive transfusion at a haemoglobin of 70 g/L governs the resuscitation.[1][3]
Definition and classification
A lower gastrointestinal bleed is any haemorrhage arising distal to the ligament of Treitz. The acute overt form presents with haematochezia — the passage of bright red or maroon blood or clots per rectum — and is the form that reaches the resuscitation bay. The occult form presents with iron-deficiency anaemia and is an outpatient workup. The obscure-overt form is visible bleeding that remains unlocalised after colonoscopy and oesophagogastroduodenoscopy, prompting capsule or deep enteroscopy. [1]
Classification is by haemodynamic severity as much as by source: a massive lower GI bleed is ongoing bleeding with haemodynamic instability (systolic blood pressure below 90 mmHg, heart rate above 100, or signs of shock). This distinction drives the entire pathway, because the massive bleed gets CT angiography and embolisation while the stable bleed gets bowel preparation and colonoscopy. The source is established at colonoscopy or angiography, not at the bedside.[1]
Epidemiology and risk
The annual incidence of acute lower GI bleeding is roughly 33 per 100,000 adults, but it rises steeply with age to nearly 200 per 100,000 in those over 65, so the typical patient is older and comorbid. The overall mortality is 2 to 4 per cent, climbing with comorbidity, anticoagulation, and an inpatient onset. The risk factors are age, anticoagulants and antiplatelets (which potentiate any source), non-steroidal anti-inflammatory drugs, prior diverticular disease, a prior lower GI bleed, chronic kidney disease, and cirrhosis. Although lower GI bleeding is commoner than upper GI bleeding in the community, the upper GI bleed carries the higher mortality, which is why the brisk upper GI bleed presenting as haematochezia is the dangerous mimic.[2]
Pathophysiology — the mechanism by source
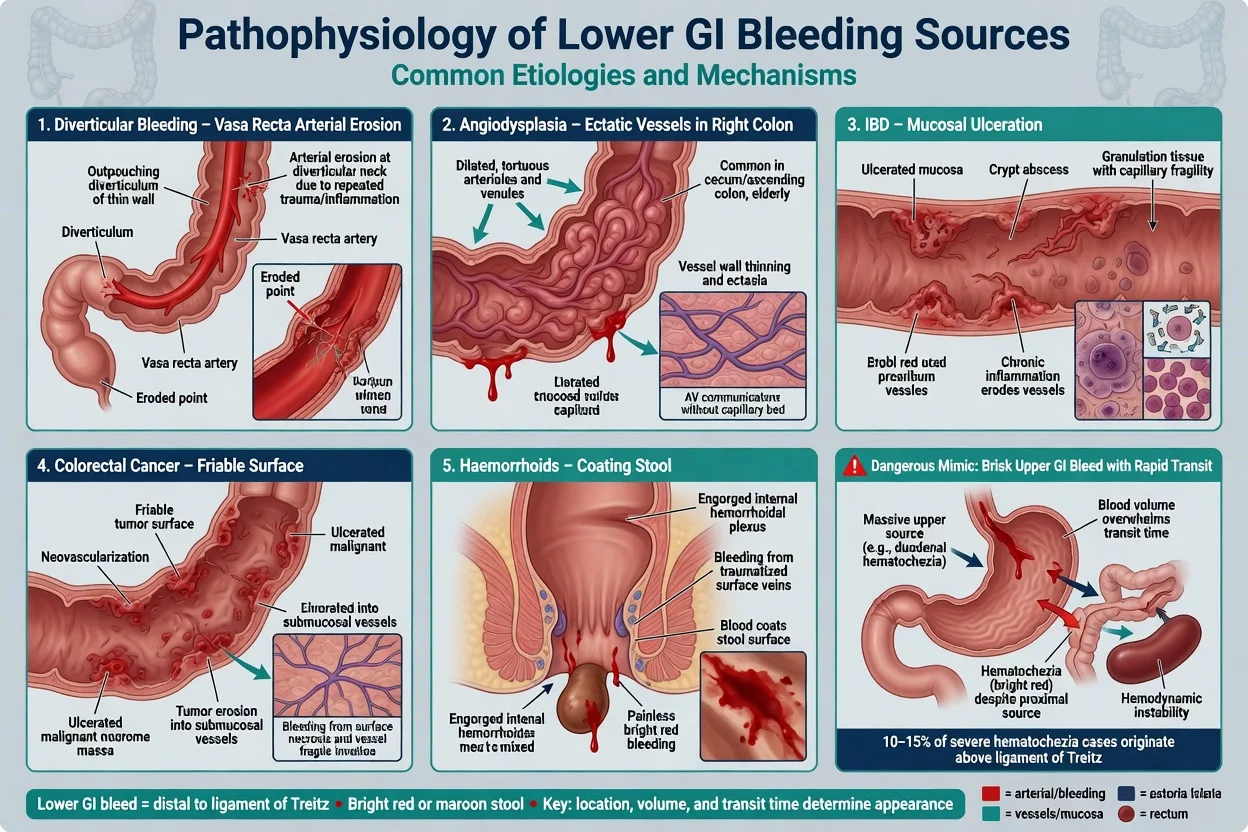
Each source bleeds by a different mechanism, and the mechanism predicts the volume and the natural history. The diverticular bleed arises when a vasa recta artery is eroded at the dome of a colonic diverticulum; it is an arterial, painless, high-volume bleed that stops spontaneously in roughly 75 to 80 per cent of patients but recurs in about a quarter. Angiodysplasia — the ectatic, dilated submucosal vessels of the caecum and ascending colon — bleeds from thin, fragile walls, typically in the elderly and those with chronic kidney disease or aortic stenosis (the Heyde syndrome). Inflammatory bowel disease produces mucosal ulceration and friable granulation tissue, presenting as bloody diarrhoea that is lower in volume but persistent and accompanied by cramps and systemic inflammation. Colorectal cancer bleeds from a friable, neovascular surface, often producing chronic occult loss but occasionally an acute bleed. Haemorrhoids arise from the dilated venous cushions of the anal canal and characteristically coat the stool with bright red blood rather than filling the bowl with clots — a distinction the bedside history must establish. [1]
Clinical presentation
The hallmark is haematochezia: bright red or maroon blood, with or without clots, passed per rectum. The diverticular and angiodysplastic bleeds are typically painless — the patient describes a sudden urge, then a toilet bowl of blood, and may report presyncope or postural dizziness. Bleeding accompanied by cramping lower abdominal pain suggests inflammatory bowel disease, ischaemic colitis, or infectious colitis. The massive bleed produces the stigmata of hypovolaemic shock — tachycardia, hypotension, cool peripheries, oliguria, and altered mental state. An atypical presentation is melaena from a slow right-colon bleed, and the single most important mimic is haematochezia from a brisk upper GI bleed with rapid transit — any patient in shock with haematochezia has an upper source until proven otherwise. [1]
Differential diagnosis — the causes and the mimics
The bedside generates the differential and the pre-test probability; the source is confirmed at endoscopy or angiography. The first task is always to exclude the brisk upper GI bleed presenting as haematochezia, because the pathway and the drugs differ completely. [1]
Upper GI bleed with rapid transit (the mimic)
- Massive haematochezia with haemodynamic compromise — the blood transits too fast to be digested
- History of peptic ulcer, cirrhosis, NSAID use; melaena may precede the red stool
- Nasogastric aspirate of blood or coffee-grounds; raised urea-to-creatinine ratio
- Goes to upper endoscopy, not colonoscopy; receives the UGIB drug bundle
Diverticular bleed (commonest)
- Painless, large-volume haematochezia in an older patient
- Arterial, vasa recta erosion; stops spontaneously in ~75 to 80 per cent
- Right-colon diverticula commoner in Asian/ANZ cohorts than Western
- Endoscopic clip or epinephrine if found; embolisation if ongoing
Angiodysplasia
- Elderly; chronic kidney disease; aortic stenosis (Heyde syndrome)
- Right colon; recurrent, often occult then acute
- Painless; may be associated with von Willebrand deficiency
- Endoscopic argon plasma coagulation; embolisation for ongoing bleed
Inflammatory bowel disease
- Bloody diarrhoea with mucus, cramps, tenesmus; younger patient
- Ulcerative colitis more than Crohn; systemic inflammation
- Lower volume but persistent; rarely massive
- Steroids, biologicals; endoscopy after stabilisation
Colorectal cancer
- Older patient; weight loss, change in bowel habit, iron-deficiency anaemia
- Friable neovascular surface; mixed acute and chronic
- Never assume the bleed is benign without full colonic visualisation
- Urgent colonoscopy and surgical referral
Ischaemic colitis
- Left-sided pain out of proportion then bloody diarrhoea; post low-flow state
- Vasculopath, recent cardiac event, dialysis, hypotension
- Watershed area (splenic flexure, rectosigmoid); peritonism = transmural
- Conservative in most; surgery if perforation or gangrene
Anorectal (haemorrhoids, fissure)
- Bright red blood coating the stool and on the paper, not mixed, not clotted
- Painless (haemorrhoid) or painful defaecation (fissure)
- Rarely massive; the digital rectal exam and proctoscopy settle it
- Outpatient referral; never accept as the cause of a massive bleed without exclusion
Other causes include the post-polypectomy bleed (typically 7 to 14 days after the procedure, from sloughing of the eschar), radiation proctitis (months to years after prostate or cervical radiotherapy), Meckel's diverticulum (the young adult with painless bleeding from ectopic gastric mucosa), and the infectious colitides (Campylobacter, Salmonella, Shigella, E. coli O157, amoebiasis — bloody diarrhoea with fever). A digital rectal examination is mandatory and confirms the presence and character of the blood. [1]
Bedside assessment
Begin with airway, breathing and circulation — the massively bleeding patient can be in established hypovolaemic shock on arrival. Attach monitoring, establish two large-bore intravenous cannulae, and set up the crossmatch while the history is taken. A focused history establishes the onset, volume, colour and frequency of the bleeding, associated pain, syncope, anticoagulant and antiplatelet use, prior colonoscopy or polypectomy, diverticular or inflammatory bowel disease, and the red-flag features of malignancy (weight loss, change in bowel habit). [1]
Examination looks for the signs of shock and end-organ hypoperfusion, palpates the abdomen for tenderness (peritonism redirects the diagnosis toward ischaemia or perforation), performs a digital rectal examination to confirm the blood and exclude an anorectal source, and screens for stigmata of chronic liver disease that would reweight the differential toward a portal-hypertensive or variceal source. A nasogastric aspirate of blood or coffee-grounds argues for an upper source and triggers upper endoscopy; a clear bilious aspirate makes an upper source unlikely but does not exclude it entirely. [1]
Investigations and risk stratification
The blood panel is the full blood count (the haemoglobin may be normal early, because haemodilution lags the bleed by 6 to 12 hours), the coagulation profile with INR (especially in the anticoagulated), the urea and creatinine (a raised urea-to-creatinine ratio points to an upper source, because digested blood is a protein load absorbed as urea), the electrolytes, the group and save with crossmatch of 2 to 4 units, and a venous lactate as the perfusion marker. An ECG and troponin are warranted in the older or cardiac-comorbid patient, because the demand ischaemia of hypovolaemia is a real contributor to mortality. [1]
The Oakland score — reproduced
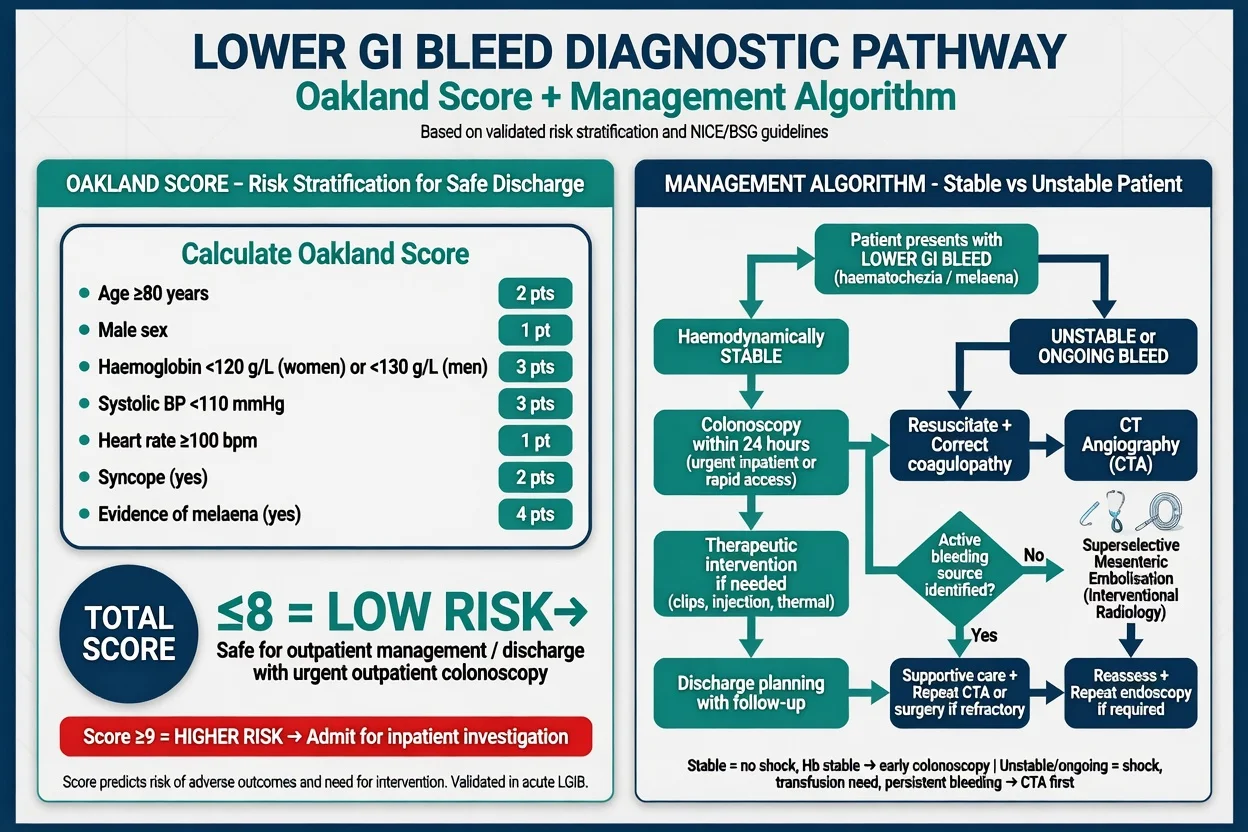
The Oakland score is the only risk-stratification tool derived specifically for the lower GI bleed, and it is the score the Fellowship examiner expects.[3] It is calculated entirely at the bedside from seven variables and predicts the composite outcome of severe bleeding — transfusion of 2 or more units, rebleeding, intervention, or death — identifying patients safe for discharge.
| Component | Value | Points |
|---|---|---|
| Age (years) | under 40 / 40 to 69 / 70 plus | 0 / 1 to 8 / 9 to 17 |
| Sex assigned at birth | male | 0 / 1 |
| Prior lower GI bleed | yes | 0 / 6 |
| Digital rectal examination | no blood | 0 / 6 |
| Systolic BP (mmHg) | up to 109 / 110 to 149 / 150 plus | 8 to 10 / 1 to 4 / 0 |
| Heart rate (per min) | up to 69 / 70 to 89 / 90 plus | 0 / 1 to 2 / 3 to 5 |
| Haemoglobin (g/L) | 130 plus / 120 to 129 / 100 to 119 / under 100 | 0 / 1 / 3 / 6 |
A score of 8 or less identifies a low-risk patient suitable for early discharge and outpatient colonoscopy. The derivation study (Oakland 2017, Lancet Gastroenterol Hepatol) reported that a score of 8 or less predicted a 95 per cent probability of safe discharge (C-statistic 0.84 development, 0.79 internal validation), outperforming the Rockall, Blatchford, Strate, BLEED, AIMS65 and NOBLADS scores.[3] The 46,000-patient US external validation (Jama Netw Open 2020) confirmed an AUROC of 0.87, with 98.4 per cent sensitivity at a threshold of 8 or less (identifying about 9 per cent of patients for safe discharge); extending to 10 captures 18 per cent at 96 per cent sensitivity.[4] The score is applied only in the stable patient; the unstable patient bypasses scoring and goes to CT angiography.
Imaging — CT angiography versus colonoscopy
The imaging strategy is governed by haemodynamic stability. The haemodynamically unstable patient with ongoing bleeding undergoes CT angiography first, because active bleeding and unprepped bowel defeat the colonoscope and the patient is too sick for a prolonged bowel preparation. CT angiography detects active contrast extravasation at bleeding rates of roughly 0.3 to 0.5 mL per minute, localises the source to a colonic segment, and directly triages the patient to therapeutic mesenteric angiography and embolisation. The haemodynamically stable patient undergoes colonoscopy within 24 hours after bowel preparation with polyethylene glycol; colonoscopy is both diagnostic and therapeutic, applying epinephrine 1:10,000 injection with clipping or argon plasma coagulation to the identified lesion. A tagged red-blood-cell scan is more sensitive (down to 0.1 mL per minute) but localises poorly and has been largely superseded by CT angiography; it retains a niche when angiography is negative but bleeding persists. Angiography with digital subtraction is both diagnostic and therapeutic — the route to superselective embolisation.[1]
Immediate management — resuscitation and restrictive transfusion
The resuscitation is the priority and runs in parallel with the workup. [1]
The restrictive transfusion strategy at a haemoglobin of 70 g/L mirrors the principle established for the upper GI bleed: the over-transfusion raises the splanchnic pressure, disrupts fresh clot, and increases rebleeding. Tranexamic acid is not recommended for lower GI bleeding — the HALT-IT trial (a 12,009-patient international randomised placebo-controlled trial) showed no reduction in death from gastrointestinal bleeding and a signal toward thromboembolic events, so it has no routine role.[6]
Definitive management — the diagnostic and therapeutic ladder
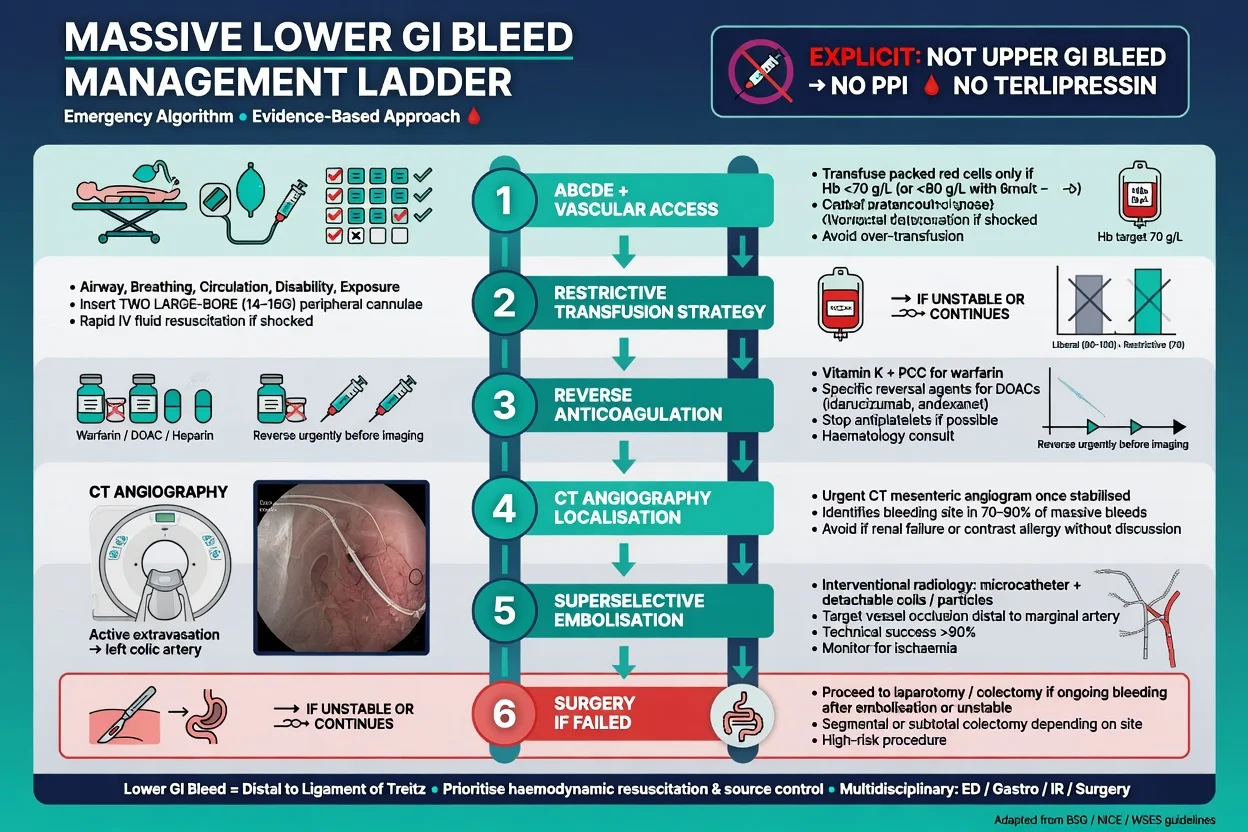
The definitive pathway is an escalation ladder governed by haemodynamic stability, and the Fellowship candidate must articulate each rung.[1][5]
- Stable, low-risk (Oakland 8 or less), no ongoing bleed: consider discharge with early outpatient colonoscopy, a clear safety-net, and return precautions (ongoing bleeding, syncope, dizziness).
- Stable with ongoing or recent bleed: colonoscopy within 24 hours after polyethylene-glycol bowel preparation. Endoscopic therapy for the diverticular or angiodysplastic lesion — epinephrine 1:10,000 injection combined with through-the-scope clipping or argon plasma coagulation.
- Unstable with ongoing bleed: CT angiography first, then superselective mesenteric angiographic embolisation — coils or particles delivered to the feeding artery. The technical success rate exceeds 90 per cent, with rebleeding in roughly 15 to 20 per cent; colonic ischaemia is uncommon at 5 to 10 per cent.[5]
- Failed or recurrent embolisation: surgery — segmental colectomy guided by the localisation, with a damage-control approach to the unstable patient.
ANZ practice note. The Australasian pathway follows the local major-haemorrhage protocol and the Gastroenterological Society of Australia guidance: ABCDE, two large-bore cannulae, crossmatch, restrictive transfusion to a haemoglobin of 70 g/L, the Oakland score for the stable patient, CT angiography for the unstable, colonoscopy within 24 hours for the stable, and superselective mesenteric embolisation for the ongoing bleed. Right-colon diverticular bleeds are proportionally commoner in Asian and Australasian cohorts than in Western cohorts. The interventional radiology and the on-call surgical teams are activated early in the massive bleed. [1]
Subtypes and scenarios
The right-colon diverticular bleed is disproportionately common in Asian and Australasian populations, in whom right-colon diverticula are more prevalent than the left-colon dominance of Western cohorts. Angiodysplasia in the elderly with chronic kidney disease or aortic stenosis (the Heyde syndrome, linked to acquired von Willebrand deficiency) tends to recur. The anticoagulated patient is reversed agent-specifically for the life-threatening bleed and resumed early once haemostasis is achieved. The post-polypectomy bleed presents 7 to 14 days after colonoscopy as the eschar sloughs; most settle with supportive care, with colonoscopy or angiography for the ongoing bleed. Radiation proctitis produces recurrent small-volume bleeding months to years after prostate or cervical radiotherapy, managed endoscopically with argon plasma coagulation. The young adult with painless bleeding has a Meckel's diverticulum until proven otherwise. [1]
Complications and pitfalls
The complications are hypovolaemic shock with end-organ failure (acute kidney injury, myocardial infarction), iatrogenic injury (post-embolisation colonic ischaemia, contrast nephropathy, post-polypectomy perforation), and rebleeding — the diverticular bleed recurs in roughly 25 per cent. The pitfalls invert good care. Treating the lower GI bleed with the upper-GI-bleed drugs — the proton pump inhibitor, the terlipressin, the prophylactic antibiotic — is a Fellowship error with no evidence. Sending the unstable patient to colonoscopy instead of CT angiography wastes the critical window. Missing the brisk upper GI bleed presenting as haematochezia in a shocked patient. Over-transfusing and provoking rebleeding. Attributing a massive bleed to the haemorrhoids in a patient with weight loss and anaemia, missing a proximal cancer. Delaying embolisation while awaiting a definitive endoscopic diagnosis in the actively bleeding patient. [1]
Prognosis and disposition
The overall mortality is 2 to 4 per cent, rising with comorbidity, anticoagulation, and an inpatient onset. The disposition follows the stability and the source. The stable, low-risk patient (Oakland 8 or less, no ongoing bleed) is discharged with outpatient colonoscopy and a safety-net. The stable with recent bleeding is admitted to the ward for colonoscopy within 24 hours. The unstable or massive bleeder is admitted to the high-dependency or intensive care unit, undergoes CT angiography and embolisation, with surgical backup. The patient with recurrent bleeding or a failed embolisation proceeds to surgery. [1]
Special populations
The anticoagulated patient has the coagulopathy as a cofactor, not the cause; reverse agent-specifically for the life-threatening bleed, identify and treat the source, and resume anticoagulation early once haemostasis is achieved. The elderly vasculopath demands exclusion of ischaemic colitis, a ruptured abdominal aortic aneurysm, and a brisk upper source. The cirrhotic patient may bleed from portal hypertensive colopathy or rectal varices, but the lower-GI pathway still applies and the variceal drugs do not. The post-polypectomy and radiation patients follow their specific pathways above. The paediatric patient with painless bleeding has a Meckel's diverticulum or a juvenile polyp until proven otherwise. [1]
Evidence and regional guidelines
The contemporary framework rests on the ACG 2023 update (Sengupta, Am J Gastroenterol): CT angiography first for the unstable patient, colonoscopy within 24 hours for the stable, restrictive transfusion to a haemoglobin of 70 g/L, no routine proton pump inhibitor, and embolisation for the ongoing bleed.[1] The original ACG 2016 guideline (Strate and Gralnek) established the diagnostic ladder.[2] The Oakland score (2017 derivation, Lancet Gastroenterol Hepatol; 2020 US external validation, JAMA Netw Open) is the only lower-GI-derived pre-endoscopic risk tool — a score of 8 or less predicts a 95 per cent probability of safe discharge in the derivation cohort and 98.4 per cent sensitivity in the 46,000-patient US validation.[3][4] Tranexamic acid is not recommended — the HALT-IT trial (Lancet 2020) showed no mortality benefit in gastrointestinal bleeding.[6] The NICE NG141 guidance (UK) parallels the ACG pathway. A 2024 meta-analysis of two decades of embolisation confirmed a technical success above 90 per cent with rebleeding in roughly 15 to 20 per cent and colonic ischaemia uncommon.[5] The Gastroenterological Society of Australia governs the local detail.
Exam pearls
- Stable gets colonoscopy within 24 hours; unstable gets CT angiography first. This single decision drives the whole station.
- The Oakland score (8 or less) identifies the patient safe for discharge — the only lower-GI-derived pre-endoscopic tool.
- Restrictive transfusion to a haemoglobin of 70 g/L — over-transfusion rebleeds.
- No proton pump inhibitor, no terlipressin, no prophylactic antibiotic in the lower GI bleed — these are upper-GI-bleed drugs.
- Haematochezia with shock is an upper GI bleed with rapid transit until proven otherwise.
- Never attribute a massive bleed to the haemorrhoids alone — the haemorrhoid coats the stool; it does not fill the bowl with clots. [1]
Model answer — the massive lower GI bleed on arrival
A 74-year-old man on apixaban for atrial fibrillation presents with a large volume of clotted haematochezia and presyncope, systolic BP 84 palp, heart rate 128, Hb 88 g/L. ABCDE: two large-bore cannulae, crossmatch 4 units, lactate, urinary catheter. Restrictive transfusion to a haemoglobin of 70 g/L — give one unit now, recheck; target 80 g/L for the ischaemic heart. Reverse the apixaban with andexanet (or prothrombin complex concentrate 25 to 50 units per kilogram if andexanet is unavailable). Activate the major-haemorrhage protocol. Do not give a proton pump inhibitor, terlipressin, or an antibiotic. CT angiography first to localise — then superselective mesenteric angiographic embolisation for the active extravasation. If embolisation fails or bleeding recurs, surgery for a damage-control segmental colectomy. Admit to the high-dependency or intensive care unit. [1]
Deep-dive — the sources, the mimics and the bedside rules
The causes by frequency — a Fellowship-ready table
The bedside generates the differential and the pre-test probability; the source is confirmed at endoscopy or angiography. The relative frequencies shift with age, but the diverticular bleed is the single commonest cause of acute overt lower GI bleeding in adults, accounting for roughly 30 to 50 per cent of presentations.[1][2]
Diverticular disease (30 to 50 per cent — commonest)
- Arterial vasa recta erosion at the diverticular dome; painless, high-volume haematochezia
- Stops spontaneously in 75 to 80 per cent; recurs in roughly 25 per cent
- Right-colon diverticula disproportionately common in Asian and Australasian cohorts
- Endoscopic clip or epinephrine; embolisation or surgery for ongoing bleed
Haemorrhoids (anorectal)
- Bright red blood coating the stool and on the paper, not mixed, not clotted
- Painless (internal haemorrhoid) or painful defaecation (fissure, thrombosed external)
- Rarely massive; digital rectal exam and proctoscopy settle it
- Never accept as the cause of a massive bleed without full colonic exclusion
Inflammatory bowel disease
- Bloody diarrhoea with mucus, cramps, tenesmus; younger patient
- Ulcerative colitis more than Crohn; systemic inflammation
- Lower volume but persistent; rarely massive
- Steroids and biologicals after stabilisation; colonoscopy once safe
Colorectal cancer
- Older patient; weight loss, change in bowel habit, iron-deficiency anaemia
- Friable neovascular surface; mixed acute and chronic loss
- Never assume the bleed is benign without full colonic visualisation
- Urgent colonoscopy and surgical referral
Angiodysplasia / AVM
- Ectatic submucosal vessels of the caecum and ascending colon; elderly
- Chronic kidney disease, aortic stenosis (Heyde syndrome), acquired von Willebrand deficiency
- Painless; recurrent, often occult then acute
- Argon plasma coagulation; embolisation for ongoing bleed
Ischaemic colitis
- Left-sided pain out of proportion then bloody diarrhoea; post low-flow state
- Vasculopath, recent cardiac event, dialysis, hypotension
- Watershed areas (splenic flexure, rectosigmoid); peritonism signals transmural infarction
- Conservative in most; surgery for perforation or gangrene
Infectious colitis
- Campylobacter, Salmonella, Shigella, E. coli O157:H7, amoebiasis
- Bloody diarrhoea with fever, abdominal cramps, recent travel or food history
- E. coli O157:H7 risks haemolytic uraemic syndrome — avoid antibiotics
- Stool culture; supportive; targeted therapy only where indicated
Meckel diverticulum (the young)
- Painless, maroon-coloured bleeding in a child or young adult
- Ectopic gastric mucosa erodes adjacent ileal mucosa
- Rule of twos: 2 per cent of population, 2 feet from ileocaecal valve, 2 inches long, age under 2 (but bleeds into young adulthood)
- Meckel scan (technetium-99m pertechnetate); segmental resection
Colonic polyps and post-polypectomy
- Friable polyp surface bleeds acutely or as chronic occult loss
- Post-polypectomy bleed presents 7 to 14 days later as the eschar sloughs
- Most settle with supportive care
- Colonoscopy or angiography for the ongoing bleed
The colour and the volume — what the stool tells you
The ED workflow — resuscitation, localisation, definitive control
The first 60 minutes of the massive lower GI bleed — the resuscitation timeline
0 to 5 minutes — ABCDE and access
Assess airway, breathing, circulation. Two large-bore (14 to 16 gauge) intravenous cannulae. Attach monitoring (ECG, oxygen saturation, non-invasive blood pressure). Call for help early; alert the major-haemorrhage protocol if shocked.
5 to 15 minutes — assess, sample, crossmatch
Focused history (onset, volume, colour, anticoagulants, prior bleed, red-flag weight loss). Examine for shock and peritonism; perform a digital rectal examination. Take blood for full blood count, coagulation, urea and electrolytes, lactate, group and crossmatch 2 to 4 units. Insert a urinary catheter and arterial line if shocked.
15 to 30 minutes — resuscitate and exclude the upper source
Balanced crystalloid 20 mL per kilogram bolus titrated to response. Restrictive transfusion to a haemoglobin of 70 g/L (80 g/L if ischaemic heart disease). Pass a nasogastric tube if an upper source is suspected — blood or coffee-grounds argues for upper endoscopy. Reverse anticoagulation agent-specifically for the life-threatening bleed.
30 to 60 minutes — image and escalate
In the unstable patient with ongoing bleeding, CT angiography first to localise active extravasation, then superselective mesenteric angiographic embolisation. In the stable patient, bowel preparation and colonoscopy within 24 hours. Activate interventional radiology, gastroenterology and surgery early in the massive bleed.
Throughout — do NOT
Do not give a proton pump inhibitor, terlipressin, octreotide, or a prophylactic antibiotic — these are upper-GI-bleed drugs with no role in the lower GI bleed. Do not send the unstable patient to colonoscopy. Do not over-transfuse.
Localising the bleed — the stability-driven diagnostic algorithm
Step 1 — is the patient stable?
Stable (no shock, no ongoing brisk bleed): proceed to risk-stratify with the Oakland score and plan colonoscopy within 24 hours. Unstable (shock, ongoing bleed): bypass scoring — go straight to CT angiography.
Step 2 — exclude the brisk upper GI source
Any shocked patient with haematochezia has an upper source until proven otherwise. A nasogastric aspirate of blood or coffee-grounds, or a raised urea-to-creatinine ratio, points upward and triggers upper endoscopy rather than colonoscopy.
Step 3 — colonoscopy for the stable
After polyethylene-glycol bowel preparation, colonoscopy within 24 hours is both diagnostic and therapeutic — epinephrine 1:10,000 injection combined with through-the-scope clipping or argon plasma coagulation for the identified lesion.
Step 4 — CT angiography for the unstable
Multidetector CT angiography detects extravasation at bleeding rates of about 0.3 to 0.5 mL per minute, localises the source to a colonic segment, and triages directly to therapeutic mesenteric angiography.
Step 5 — tagged RBC scan (the niche)
A technetium-99m labelled red-blood-cell scan detects bleeding down to 0.1 mL per minute but localises poorly; it retains a niche when CT angiography is negative but bleeding persists, and can guide angiography timing.
Step 6 — surgery for refractory bleeding
Failed or recurrent embolisation, or a surgically correctable lesion (cancer, Meckel diverticulum), proceeds to segmental colectomy guided by the localisation — damage-control in the unstable.
Agent-specific anticoagulation reversal in the life-threatening lower GI bleed
Warfarin
Vitamin K 5 to 10 mg intravenously plus prothrombin complex concentrate 25 to 50 units per kilogram for the life-threatening bleed. Recheck the INR at 30 minutes. Fresh frozen plasma only if prothrombin complex concentrate is unavailable.
Dabigatran
Idarucizumab 5 g intravenously (two 2.5 g vials). The specific, immediate reversal. Activated charcoal within 2 hours if recently ingested.
Apixaban or rivaroxaban (factor Xa inhibitors)
Andexanet alfa where available; otherwise prothrombin complex concentrate 25 to 50 units per kilogram. Activated charcoal within 2 hours if recently ingested.
Antiplatelets (aspirin, clopidogrel)
Hold for the acute bleed; platelet transfusion is generally reserved for the actively bleeding patient on antiplatelet agents with thrombocytopenia or planned surgery. Resume early once haemostasis is achieved.
Heparin and low-molecular-weight heparin
Stop the infusion (heparin half-life about 60 to 90 minutes). Protamine sulphate 1 mg per 100 units of heparin for the life-threatening bleed (partial reversal of low-molecular-weight heparin).
Resume early
The anticoagulant is a cofactor, not the cause. Identify and treat the source, then resume anticoagulation as soon as haemostasis is secure — the thromboembolic risk of interruption often exceeds the rebleeding risk of resumption.
Imaging comparison — choosing the modality
Colonoscopy (the stable patient)
- Diagnostic AND therapeutic — clip, epinephrine, argon plasma coagulation
- Requires bowel preparation with polyethylene glycol; performed within 24 hours
- Yields the definitive source and allows biopsy of cancer or colitis
- Contraindicated in the unprepped, actively bleeding, unstable patient
CT angiography (the unstable patient)
- First-line for the haemodynamically unstable, ongoing bleed
- Detects extravasation at bleeding rates of about 0.3 to 0.5 mL per minute
- Rapid; localises to a colonic segment; triages to therapeutic angiography
- No bowel preparation needed; safe in the unprepped bowel
Mesenteric angiography (therapeutic)
- Both diagnostic and therapeutic — superselective coil or particle embolisation
- Technical success above 90 per cent; rebleeding in 15 to 20 per cent
- Colonic ischaemia uncommon (5 to 10 per cent); contrast nephropathy a risk
- Used after positive CT angiography, or for the refractory bleed
Tagged red-blood-cell scan (the niche)
- Most sensitive — detects bleeding down to 0.1 mL per minute
- Poor anatomical localisation; high false-positive and false-localisation rate
- Largely superseded by CT angiography
- Retained role when CT angiography is negative but bleeding persists
Source-specific pearls
The management ladder — colonoscopic to surgical
The escalation ladder for the ongoing lower GI bleed
Rung 1 — stable and low-risk (Oakland 8 or less)
Discharge with a clear safety-net and return precautions (ongoing bleeding, syncope, dizziness) and arrange early outpatient colonoscopy.
Rung 2 — stable with recent or ongoing bleed
Admit; bowel preparation with polyethylene glycol; colonoscopy within 24 hours. Endoscopic therapy — epinephrine 1:10,000 injection with through-the-scope clipping or argon plasma coagulation.
Rung 3 — unstable with ongoing bleed
CT angiography first to localise active extravasation; superselective mesenteric angiographic embolisation with coils or particles. Technical success above 90 per cent; rebleeding 15 to 20 per cent.
Rung 4 — failed or recurrent embolisation
Surgery — segmental colectomy guided by the localisation, with a damage-control approach to the unstable patient (resection, temporary closure, physiology first).
Rung 5 — recurrent and unlocalised
Intraoperative enteroscopy or on-table colonoscopy to localise; subtotal colectomy reserved for the truly unlocalised, exsanguinating bleed after upper and lower endoscopy have failed.
Landmark evidence and trials
ACG 2023 — Management of acute lower GI bleeding (Sengupta, Am J Gastroenterol 2023)
Source
American College of Gastroenterology updated guideline — the contemporary standard
Key recommendations
CT angiography first for the unstable patient; colonoscopy within 24 hours for the stable; restrictive transfusion to a haemoglobin of 70 g/L; no routine proton pump inhibitor; embolisation for the ongoing bleed
Risk tool
Endorses the Oakland score to identify low-risk patients suitable for early discharge and outpatient colonoscopy
Clinical bottom line
The framework the Fellowship candidate must articulate — stability drives imaging, restrictive transfusion governs resuscitation, and the upper-GI-bleed drugs have no role
Oakland 2017 — derivation of the Oakland score (Lancet Gastroenterol Hepatol)
Design
Multivariable logistic regression on 2,336 prospectively identified UK admissions across 143 hospitals (National Comparative Audit of Lower Gastrointestinal Bleeding), externally validated in 288 patients
Variables
Seven bedside variables — age, sex, prior lower GI bleed, rectal examination findings, heart rate, systolic blood pressure, haemoglobin
Performance
C-statistic 0.84 (development) and 0.79 (validation); outperformed Rockall, Blatchford, Strate, BLEED, AIMS65 and NOBLADS scores
Clinical bottom line
A score of 8 or less predicts a 95 per cent probability of safe discharge — the only lower-GI-derived pre-endoscopic risk tool
Oakland 2020 — US external validation (Oakland, JAMA Netw Open)
Design
Multicentre prognostic study of 38,067 adult patients with lower GI bleeding across 140 US hospitals (HCA network)
Performance
AUROC 0.87 for safe discharge; at a threshold of 8 or less, sensitivity 98.4 per cent (identifying 8.7 per cent of patients); extending to 10 captures 17.8 per cent at 96 per cent sensitivity
Safe discharge
Defined as no blood transfusion, rebleeding, haemostatic intervention, readmission, or death
Clinical bottom line
Confirms the Oakland score robustly identifies low-risk patients; the threshold may be extended from 8 to 10 to safely discharge a greater proportion
HALT-IT 2020 — tranexamic acid in gastrointestinal bleeding (Lancet)
Design
International, randomised, double-blind, placebo-controlled trial of 12,009 patients with acute gastrointestinal bleeding
Intervention
Tranexamic acid 1 g intravenous loading dose then 3 g over 24 hours, versus placebo
Result
No reduction in death from bleeding (3.7 per cent tranexamic acid vs 3.8 per cent placebo); a signal toward more venous thromboembolic events and seizures with tranexamic acid
Clinical bottom line
Tranexamic acid has no routine role in gastrointestinal bleeding, upper or lower — do not give it for the lower GI bleed
Yu 2024 — two decades of embolisation for acute lower GI bleeding (Br J Radiol)
Design
Meta-analysis of superselective mesenteric angiographic embolisation for acute lower GI bleeding over twenty years
Technical success
Above 90 per cent — embolisation reliably achieves immediate haemostasis
Rebleeding and ischaemia
Rebleeding in roughly 15 to 20 per cent; colonic ischaemia uncommon at 5 to 10 per cent
Clinical bottom line
Embolisation is the first-line definitive therapy for the unstable or ongoing lower GI bleed after CT angiography localisation, with surgery held in reserve
SAQ — Massive haematochezia with apixaban: resuscitation bundle and reversal
12 minutes · 10 marks
A 76-year-old man with non-valvular atrial fibrillation on apixaban 5 mg twice daily, hypertension, ischaemic heart disease and stage 3 chronic kidney disease (eGFR 38 mL/min/1.73 m²) presents to the ED with two episodes of large-volume bright-red haematochezia with clots over the past hour, presyncope on standing, and one further passage of maroon blood in the resuscitation bay. Observations: GCS 15, T 36.8, HR 124, BP 88/54 (palp), RR 22, SpO₂ 96% room air. Cool peripheries, capillary refill 4 seconds, mucous membranes dry. Abdomen soft, non-tender, no peritonism, fresh blood on the glove on digital rectal examination. Labs drawn: Hb 92 g/L, INR 1.1, APTT 32 s, platelets 215, urea 11.2 mmol/L, creatinine 168 µmol/L, lactate 4.6 mmol/L, group O-negative uncrossmatched available. The patient is awaiting CT angiography. He received his last apixaban dose six hours ago.
SAQ — Stable lower GI bleed: Oakland score calculation and investigation pathway
12 minutes · 10 marks
A 62-year-old previously well woman presents with three small-volume passages of bright-red blood coating the stool over the past 12 hours, no clots, no melaena, no abdominal pain, no syncope. She takes no anticoagulants or antiplatelets, has no prior colonoscopy. Observations: GCS 15, T 36.6, HR 78, BP 142/86, RR 16, SpO₂ 99% room air. Abdomen soft, non-tender. Digital rectal examination confirms fresh blood on the glove but no mass. Labs: Hb 118 g/L, platelets 240, INR 1.0, urea 5.4 mmol/L, creatinine 76 µmol/L, lactate 1.1 mmol/L. She is haemodynamically stable, no signs of shock, and the bleeding has settled. Her past medical history includes a previous sigmoid resection for diverticular disease and no history of malignancy. Bowel sounds are normal; there is no family history of bowel cancer.
Red flags
[1]References
- [1]Sengupta N, Cannon ML, Tavan RT, et al. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline Am J Gastroenterol, 2023.PMID 36735555
- [2]Strate LL, Gralnek IM. ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding Am J Gastroenterol, 2016.PMID 26925883
- [3]Oakland K, Jairath V, Uberoi R, et al. Derivation and validation of a novel risk score for safe discharge after acute lower gastrointestinal bleeding: a modelling study Lancet Gastroenterol Hepatol, 2017.PMID 28651935
- [4]Oakland K, Kothiwale S, Forehand T, et al. External Validation of the Oakland Score to Assess Safe Hospital Discharge Among Adult Patients With Acute Lower Gastrointestinal Bleeding in the US JAMA Netw Open, 2020.PMID 32633766
- [5]Yu Q, Hu Y, Fu K, et al. Twenty years of embolization for acute lower gastrointestinal bleeding: a meta-analysis of rebleeding and ischaemia rates Br J Radiol, 2024.PMID 38364312
- [6]HALT-IT Trial Collaborators Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial Lancet, 2020.PMID 32563378