EM · Procedural & diagnostic ED skills
Wound closure and suturing techniques
Also known as Suturing · Suture techniques · Wound closure · Tissue adhesive · Dermabond · Steri-strips · Subcuticular suture · Mattress suture
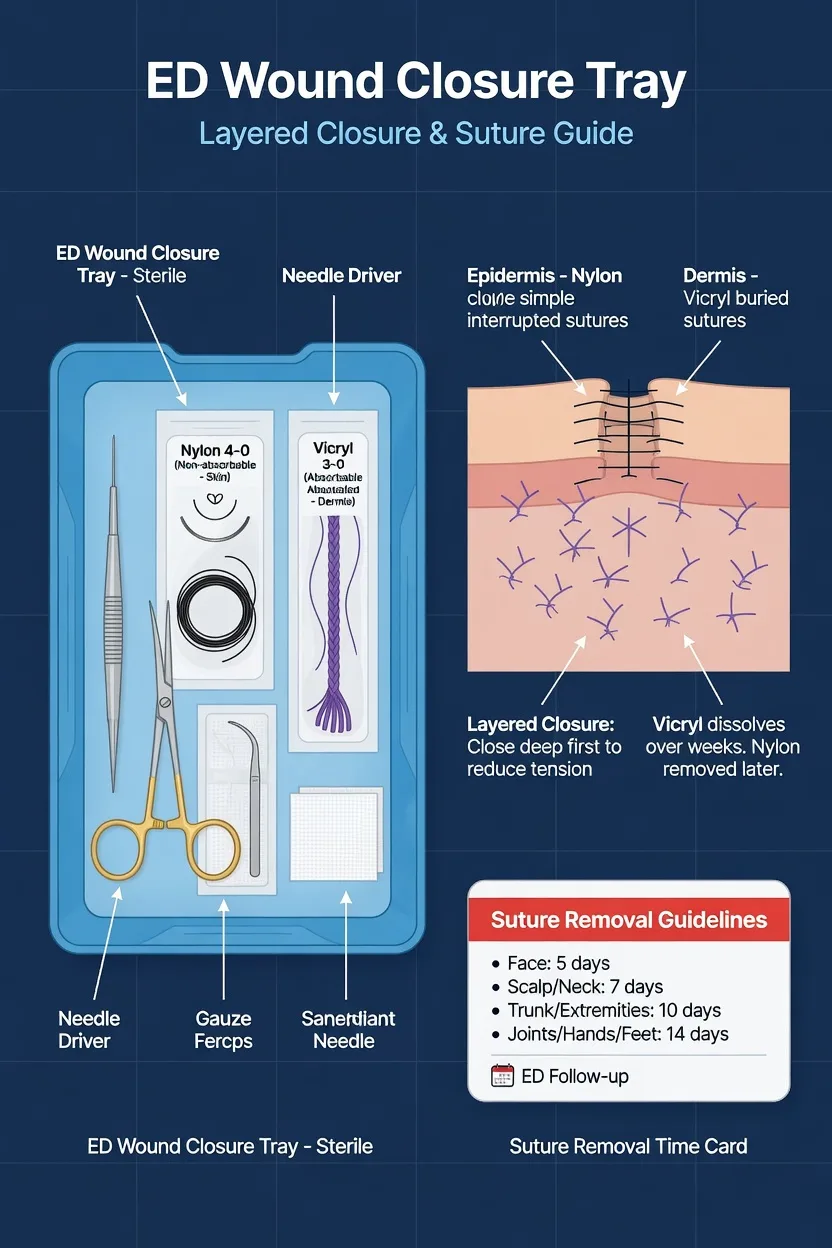
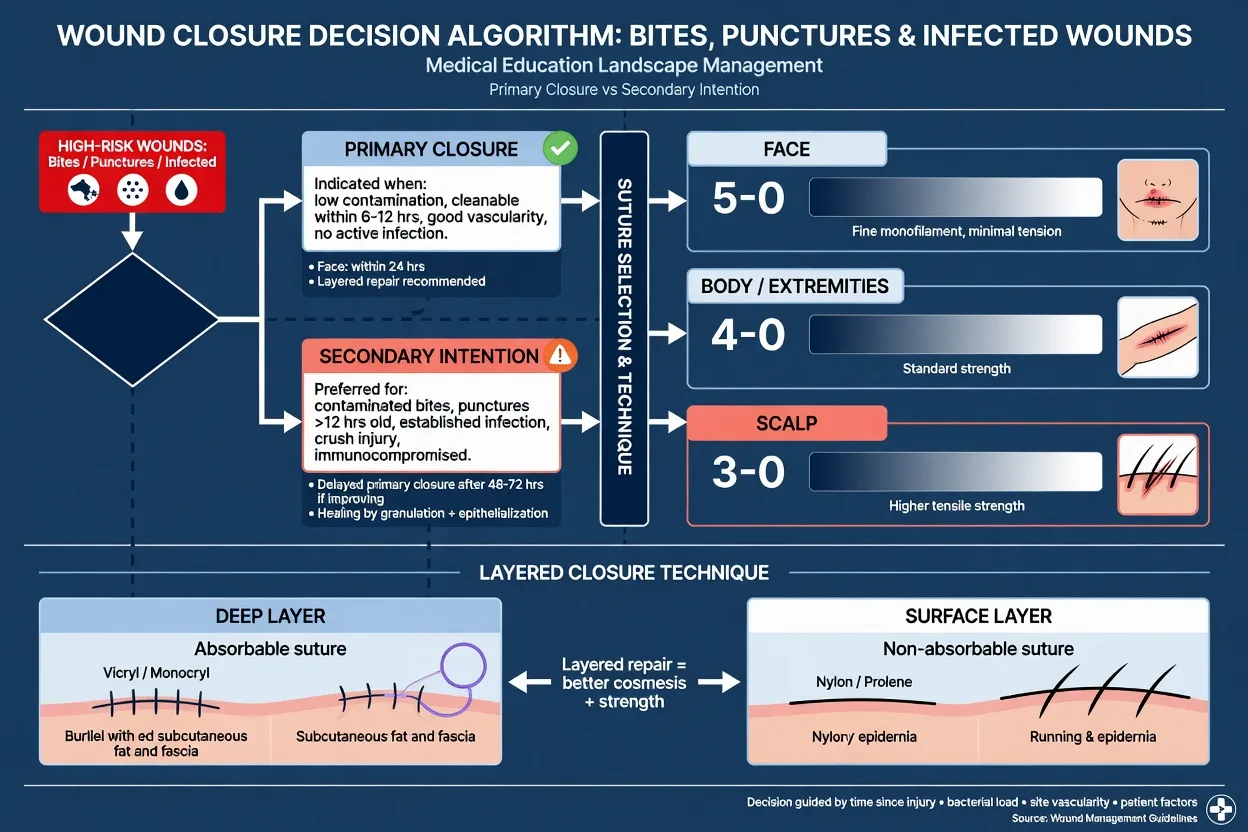
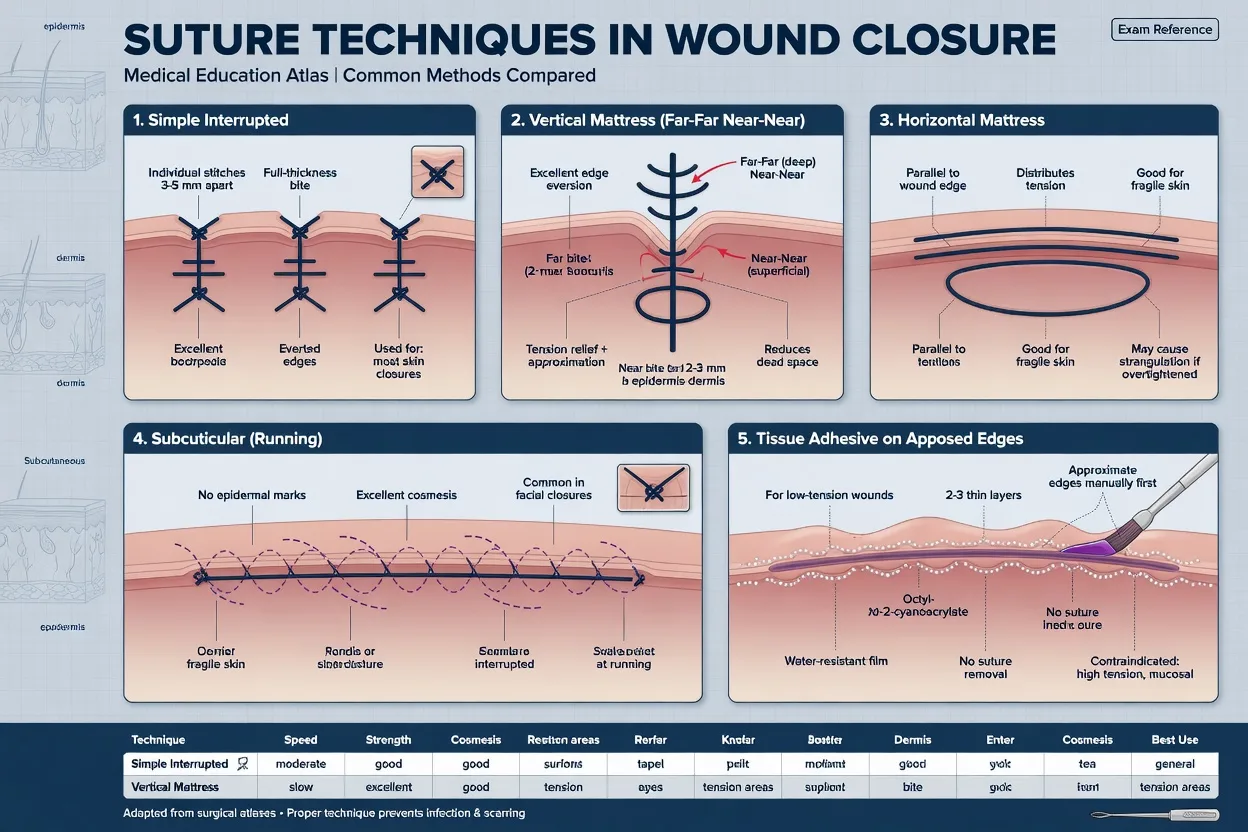
Wound closure and suturing techniques in the ED — the suture material choice (absorbable: catgut, Vicryl polyglactin, Monocryl poliglecaprone; versus non-absorbable: nylon Ethilon, polypropylene Prolene), the gauge-by-site rule (5-0 for the face, 4-0 for the body, 3-0 for the scalp and extremity), the five core techniques (simple interrupted, continuous running, vertical mattress, horizontal mattress, subcuticular intradermal) with the indication and the pitfall of each, the tissue adhesive (2-octyl cyanoacrylate, Dermabond) and adhesive strips (Steri-Strips) for the low-tension low-risk wound, the suture removal schedule (face 5 days, scalp 7 to 10, body 7 to 10, joints 14), the local anaesthetic doses for painless closure, and the recognition of the wound that must heal by secondary intention (bites, punctures, infected and heavily contaminated wounds). ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
5 MCQs with explanations
Target exams
Red flags
Wound closure is the practical craft of emergency medicine — the procedural skill the Fellowship examiner tests directly in the OSCE and in any laceration SAQ. The candidate must hold three decisions at once: which material (absorbable versus non-absorbable, and the gauge), which technique (interrupted, continuous, mattress, subcuticular, tissue adhesive, adhesive strips), and which wound to close at all — because the wrong closure on a contaminated wound converts a low-risk laceration into a deep infection. Closure is the last step of a wound that has already been assessed, irrigated and debrided; this topic assumes that work is done (see the wound assessment topic) and concentrates on the closure itself. The bar is that a candidate who has read only this topic could deliver a laceration repair in an OSCE station, defend the suture choice in a viva, and answer any SCQ on closure method and removal interval.[1][10]
Indications and the principle of edge-to-edge apposition
The indication for surgical closure is a clean or clean-contaminated laceration whose edges can be approximated without excessive tension and without trapping contamination. The biological goal of every closure is the same: bring healthy, well-vascularised, bleeding edges into contact so that the four phases of healing (haemostasis, inflammation, proliferation, remodelling) can occur across a narrow gap. A wound approximated over devitalised tissue, foreign material or a haematoma fails — it dehisces or infects. The mechanical goal is precise apposition with slight eversion of the edges, because eversion compensates for the wound contraction that flattens the scar over the following weeks; a flat or inverted edge heals to a depressed scar that the patient will see for life on the face. [1]
Closure is worthwhile only when it produces a better outcome than healing by secondary intention, which means a faster heal, a smaller scar, and a lower infection risk for the appropriate wound. For the clean facial laceration seen within hours, closure is clearly superior. For the bite, the puncture, the infected wound and the heavily contaminated crush, closure is harmful — these heal by secondary intention (see the Differential section).[1][10]
Contraindications — the wound that must NOT be closed
The contraindications are the wounds in which closure traps bacteria in a space the host cannot clear, or in which the tissue is too devitalised to hold a stitch. The Fellowship candidate must name these out loud in the OSCE before picking up the needle driver, because closing a contraindicated wound is the single most dangerous error in laceration repair. [1]
- Mammalian bites (dog, cat, human) — inoculated with oral flora; infection rates 10 to 50 per cent if closed. Clean, irrigate, leave open or delayed primary, antibiotics.
- Puncture wounds — a narrow tract that cannot be irrigated to its depth; closing it seals the contaminant in.
- Infected wounds (pus, cellulitis, abscess) — closing an infected wound creates an abscess; open and drain.
- Heavily contaminated or devitalised wounds with extensive tissue loss — these need debridement and delayed primary or secondary intention.
- Wounds over 6 to 24 hours old on high-tension, high-bacterial-load sites (hands, feet, extremities) — the closure decision integrates age with site and host; the rigid 6-hour golden period is contested, but old contaminated extremity wounds are still high-risk.[10]
- Cosmetic sites beyond ED scope — complex facial lacerations involving the vermillion border, eyelid margin, nasolacrimal duct or facial nerve are referred to plastics.
Relevant anatomy, skin tension lines and suture physics
Closure rests on the skin's layered anatomy — epidermis, dermis, subcutaneous fat, fascia — and on the principle that deep, tension-bearing layers take the load off the surface suture. A laceration through skin and subcutaneous tissue needs a deep (dermal) absorbable layer to remove tension, followed by a surface non-absorbable layer for precise epidermal apposition. Closing only the surface under tension guarantees cutting through tissue and dehiscence. [1]
The skin tension lines (Langer lines, refined as the relaxed skin tension lines, or RSTLs) run circumferentially around joints and perpendicular to the long axis of underlying muscle. A laceration parallel to the RSTL is low-tension and scars well; a laceration perpendicular to it is high-tension and scars poorly. The mattress sutures and a deeper dermal layer exist precisely to neutralise tension across a laceration that lies at right angles to the tension lines. [1]
The United States Pharmacopeia (USP) suture gauge runs inversely to the diameter: more zeros means a finer suture. A 5-0 suture is finer than a 3-0, which is finer than a 0. The choice balances tensile strength (must hold the wound), tissue reaction (less is better on the face), and capillarity (multifilament braided sutures wick fluid and bacteria into the wound and are not used on skin surfaces). The two properties that govern handling are memory (the tendency of a monofilament to return to its packaged curl, which makes nylon and polypropylene harder to handle than braided silk) and knot security (the number of throws needed to stop the knot slipping — monofilaments need more throws than braided).[1]
Equipment and the suture pack
The laceration tray holds a defined set: a needle driver (held in the non-dominant hand for a right-hander, with the needle grasped at the tip two-thirds from the swage), toothed Adson forceps (toothed, to grip tissue without crushing — non-toothed forceps crush and devitalise), tissue scissors (iris or tenotomy) and suture scissors, a scalpel with a number 15 blade for debridement, a syringe and needle for local anaesthesia, sterile gauze, and the chosen suture packet. The suture packet itself declares three facts the candidate must read aloud: the material (e.g. polyamide = nylon), the gauge (e.g. 5-0), and the needle (a cutting or reverse-cutting needle for skin; taper for viscera). Reverse-cutting needles are preferred for skin because the flat edge sits against the wound edge, reducing the chance of the needle cutting out and of a triangular tissue tear. The candidate must be able to name every instrument in the OSCE when the examiner points at it. [1]
Suture materials — absorbable versus non-absorbable
The material decision splits on whether the suture holds its strength long enough to need removal. Non-absorbable sutures retain tensile strength beyond 60 days and are removed; they are the default for the skin surface. Absorbable sutures lose tensile strength within 60 days and are hydrolysed or proteolysed in tissue; they are the default for deep dermal layers, mucosa and paediatric skin where removal is difficult or distressing. [1]
The evidence that absorbable sutures are acceptable on the paediatric face is decisive: Luck's randomised comparison of absorbable Vicryl versus non-absorbable nylon for paediatric facial lacerations found no difference in cosmetic outcome at long-term follow-up, and absorbable closure spared the child a removal visit.[2][3] This is the answer the examiner rewards for the OSCE stem of the distressed child with a facial laceration — an absorbable surface suture, or tissue adhesive, spares removal trauma without sacrificing cosmetic outcome.
Suture gauge selection by site
The gauge is matched to the tissue: the face needs the finest suture that will hold (cosmetic priority, low tension), while the scalp and extremities need a heavier suture (tension and vascularity). The candidate must produce the standard mapping without hesitation. [1]
The suture gauge by anatomical site
The pitfall is the too-fine suture under tension: a 6-0 suture on a pretibial laceration will cut through the oedematous skin and the wound will dehisce. The reverse pitfall is the too-heavy suture on the face: a 3-0 suture on a cheek laceration leaves a cross-hatched scar the patient cannot hide. Match the gauge to the site, and when tension is high add a deep absorbable layer rather than upsizing the surface suture. [1]
Patient preparation, consent and local anaesthesia
Preparation is the same four steps for every closure: document the neurovascular and tendon examination BEFORE injecting local anaesthetic (anaesthesia abolishes the chance to re-test and a missed digital nerve or tendon is the medicolegal trap), obtain informed consent (the procedure, the material, the scar, infection, dehiscence, the removal interval), position the patient supine with good lighting and the wound at the operator's eye level, and prep the skin with chlorhexidine or povidone-iodine around (not into) the wound bed. [1]
Local anaesthesia is covered in its own topic; the doses the closure operator must know are lidocaine 1 per cent 3 mg/kg plain (7 mg/kg with adrenaline), with a 25- to 30-gauge needle, injected slowly through the wound edge (less painful than through intact skin), buffered with sodium bicarbonate 9:1 to halve injection pain, and warmed to body temperature. Adrenaline-containing solution is never injected into an end-artery territory (fingers, toes, nose tip, pinna, penis). For the distressed child, LET gel (lidocaine-epinephrine-tetracaine) instilled into the wound for 20 to 30 minutes provides needle-free anaesthesia and converts many repairs. [1]
Stepwise technique — the simple interrupted suture
The simple interrupted suture is the default closure and the technique the OSCE examiner watches most closely. The first step is adequate local anaesthesia — infiltrate lidocaine 1 per cent to a maximum of 3 mg/kg plain (7 mg/kg with adrenaline), buffered 9:1 with sodium bicarbonate and injected slowly through the wound edge, waiting 5 minutes for onset before the first bite. The closure itself is run to a fixed sequence so that no step is missed. [1]
The simple interrupted suture sequence, in order
- Evert the edge — with the toothed forceps, lift the wound edge so the needle enters perpendicular to the skin surface; the bite must include dermis to allow eversion.
- Enter the needle 90 degrees to the skin — drive the needle through by supinating the wrist, following the curve of the needle so the tissue is parted, not cut.
- Equal depth and distance — the bite should be the same distance from the wound edge on each side and the same depth, so the edges meet squarely; an unequal bite inverts the wound.
- Throw a square knot — four to five throws for a monofilament (which has poor knot security), tying just tight enough to appose without blanching the skin; a granny knot or a too-tight knot strangulates tissue.
- Cut the ends — leave a 2 to 3 mm tail for non-absorbable (so removal can find the knot) or cut flush and buried for absorbable subcuticular.
- Space the sutures — place the next suture at a distance equal to the bite width from the last; check that the wound stays everted after each throw. [1]
The two structural errors are the inverted wound (a depressed scar — the commonest avoidable cosmetic defect, prevented by perpendicular entry and a dermal bite) and the too-tight first throw (tissue blanching then necrosis under the suture, a strangulating cross-hatch scar). The principle "approximate, do not strangulate" is the rule the examiner rewards.[1]
The continuous (running) suture
The continuous or running suture is placed as a single thread that loops across the wound, anchoring at each end with a knot. Its strengths are speed (half the time of interrupted), even tension distribution, and a tidy look for long, straight, low-tension lacerations. Its weaknesses are that one break or one loose throw unravels the whole closure (a single point of failure), it is less precise for irregular wounds, and it cannot be selectively loosened if one segment swells. The continuous suture is the choice for a long, clean, straight laceration on a flat surface (a forearm or flank laceration) where speed matters; it is avoided on irregular, high-tension or contaminated wounds where a selective failure would be catastrophic. The locking variant (running locked) gives extra haemostasis and is used on vascular tissues such as the scalp. [1]
Mattress sutures — vertical and horizontal
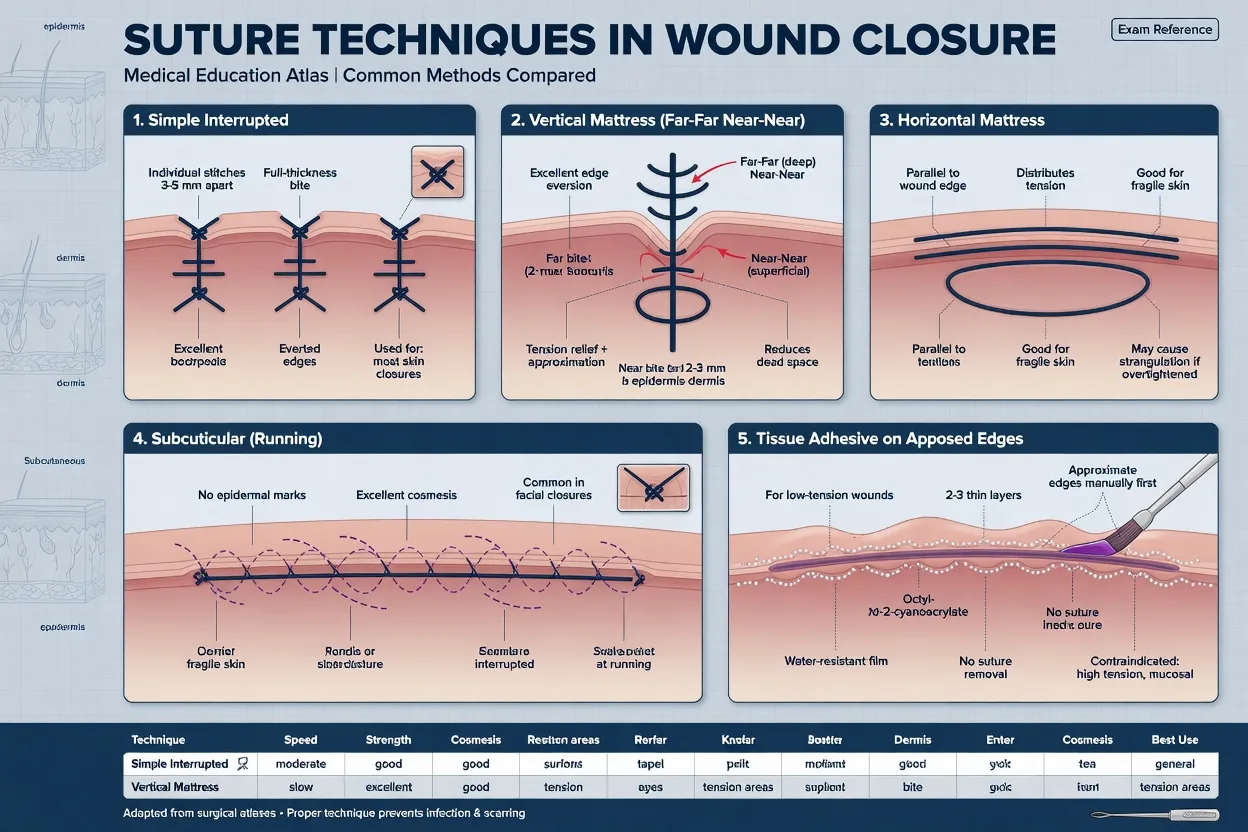
The mattress sutures are the tension-and-eversion techniques. They are placed as a deep-and-superficial pair that bites widely and everts the wound deliberately, and they are the answer to the SCQ on "best closure for a high-tension laceration" or "best closure to evert a bevelled edge". [1]
Vertical mattress
- A deep bite far from the edge followed by a superficial bite close to the edge, in the same plane perpendicular to the wound — the classic "far-far, near-near"
- Best for high-tension wounds (pretibial, extensor extremity, over a joint) and for everting a wound that keeps rolling inward
- Everts and takes tension off the surface suture; the deep throw apposes dermis, the superficial throw aligns the epidermis
- Pitfall: leave the knot loose enough that the skin is not blanched, or the cross-hatch scar is severe; remove at the longer interval for the site
Horizontal mattress
- Two bites on the same side parallel to the wound edge, then two on the opposite side — throws lie parallel to the wound
- Best for everting a difficult edge (a bevelled or thin-flap laceration) and for distributing tension across a wider band of tissue
- Bites parallel to the wound, so it everts without deep tension; useful on the scalp and on intercostal closures
- Pitfall: greater strangulation risk than vertical mattress because the loop lies across the skin surface — under-tighten, and remove early to avoid cross-hatching
The discriminator the examiner rewards: vertical mattress for high tension and deep dermis apposition (far-far near-near perpendicular to the wound), horizontal mattress for eversion of a difficult edge (parallel to the wound, wider surface distribution). Both cross-hatch badly if left too long, so a buried absorbable deep layer plus a fine surface suture is preferred wherever cosmetic outcome matters. [1]
Subcuticular (intradermal) suture
The subcuticular suture runs within the dermal layer parallel to the skin surface, entering and exiting at the wound ends, with each bite taking the dermis on alternating sides so the edges are pulled together beneath the epidermis. It produces the best cosmetic result because no suture crosses the skin surface — there is no cross-hatching and no surface knot — and it can be left in place as an absorbable Monocryl without removal. The subcuticular closure is the choice for elective or clean surgical incisions and for cosmetically critical facial closures where a plastic cosmetic outcome is the goal. Its limitation is that it requires a clean, low-tension wound with healthy dermis to bite into, and the technique takes longer than interrupted. A non-absorbable subcuticular suture (with beads or anchors at each end) is pulled out at removal; an absorbable subcuticular (Monocryl) is left to dissolve. The randomised comparison of Steri-Strip versus subcuticular closure for paediatric groin wounds found equivalent cosmetic outcomes, supporting adhesive strips as a needle-free alternative where the wound is low-tension.[11]
Tissue adhesive and adhesive strips
The needle-free closures — tissue adhesive (2-octyl cyanoacrylate, Dermabond) and adhesive strips (Steri-Strips) — are first-line for the small, low-tension, low-contamination laceration, especially in children, where they spare the needle, the removal visit and the cross-hatch scar. The systematic reviews and randomised trials establish that, for the appropriate wound, they give cosmetic outcomes equivalent to sutures at lower cost and less pain.[4][8][9]
The tissue-adhesive evidence is broad: Farion's systematic review of randomised trials established equivalence to sutures for the appropriate wound with lower procedure time and less pain, and the cost-effectiveness trial confirmed lower cost per closure.[4][9] Specific paediatric uses extend the role — tongue lacerations repaired with Dermabond, nail-bed injuries closed with adhesive rather than suture, and guardian-rated cosmetic outcomes equivalent to absorbable suture.[5][6][7] The principle unifying these is that the wound must be low-tension, clean, and on a surface that does not move: the candidate who glues a finger or a knee has chosen the wrong closure, because flexion shears the polymer off and the wound opens.
Differential diagnosis — which wound to close, which to leave
The Fellowship decision point is recognising the wound that should NOT be closed — the wound that must heal by secondary intention. The candidate must distinguish these out loud before reaching for the needle driver. [1]
Primary closure (suture or adhesive)
- Clean and clean-contaminated lacerations, low tension, healthy host, seen within hours
- Sharp lacerations (glass, knife) with clean edges; facial lacerations (cosmetic priority, low infection risk); many paediatric lacerations
- The default for the wound that will heal by first intention — fastest heal, smallest scar, lowest infection
- Suture, tissue adhesive or adhesive strips per site and tension
Delayed primary closure
- Contaminated wounds that are cleanable but not safe to close at presentation — cleaned, debrided, dressed open, then closed on day 4 to 5
- Crush and heavily contaminated lacerations; old wounds on extremities; wounds with questionably viable tissue
- The delay lets host defence and irrigation reduce the inoculum; closing on day 4 to 5 captures first-intention healing once the bacterial load is controlled
- Indicated for the wound too contaminated to close now but not infected
Secondary intention (heal by granulation)
- Mammalian bites, puncture wounds, infected wounds, abscess cavities, wounds with extensive tissue loss
- Heal by granulation, contraction and epithelialisation over weeks — larger scar but the lowest infection risk because no tissue is approximated over bacteria
- NEVER suture these in the ED — closing traps inoculated oral flora (bites) or sealed-in contamination (punctures) and drives deep infection
- Clean, irrigate, debride, dress, antibiotics per the wound type; surgical review for the deep or necrotic wound
The discriminating question on every wound is the same: does closing this wound trap bacteria in a space I cannot irrigate? If yes — the bite, the puncture, the abscess — the wound heals by secondary intention.[10]
Suture removal — the timing by site
Suture removal is timed to the balance between gaining enough tensile strength to stay closed and minimising cross-hatch scarring from sutures left too long. The face heals fastest and scars most visibly, so face sutures come out early; joints heal slowest under constant motion, so joint sutures stay longest. [1]
The suture removal schedule by site
The pitfall is leaving face sutures too long (cross-hatch) or removing joint sutures too early (dehiscence). For the high-tension wound (over a joint, the pretibial surface, the back), reinforce with adhesive strips after removal to protect the immature scar for a further week. Absorbable sutures, tissue adhesive and adhesive strips do not require removal — they dissolve or slough off — which is their chief advantage in children and in patients unlikely to return.[2]
Complications and pitfalls
The complications fall into closure-related and host-related groups. Infection is the commonest — risk rises with contamination, age over 6 hours, extremity location, diabetes, immunosuppression and retained foreign body. Dehiscence follows excessive tension, premature removal, infection, or a too-fine suture cutting through tissue. Cross-hatch (train-track) scarring follows sutures left too long or tied too tight. Hypertrophic and keloid scars are more common in darker skin types and over the sternum, shoulders and upper arms; counsel the patient and offer silicone gel and early plastic review. Retained suture is the late pitfall of a deeply-buried absorbable that does not dissolve, or a non-absorbable knot left in. Needlestick injury to the operator is the procedural hazard — never re-cap, always use the needle holder and forceps, and report a blood-borne-virus exposure immediately for post-exposure prophylaxis. [1]
The pitfalls invert the structure: closing a bite or puncture (the classic error); the too-fine suture under tension (dehiscence); the inverted wound (depressed scar from a flat or unequal bite); strangulating tension on the first throw (necrosis and cross-hatch); placing tissue adhesive inside the wound (cytotoxic); gluing a finger or a knee (flexion shears it off); leaving face sutures beyond 5 days (cross-hatch); removing joint sutures before 14 days (dehiscence); failing to document the pre-anaesthesia neurovascular check; and forgetting the safety-net — discharge advice to return for spreading redness, increasing pain, fever, or a wound that opens. [1]
Post-procedure care and disposition
After closure, the wound is dressed with a non-adherent dressing (paraffin gauze or a semi-occlusive film) and a light bandage for the first 24 to 48 hours, kept clean and dry. The patient is discharged with the removal interval written down (face 5 days, scalp 7 to 10, body 7 to 10, joints 14), advice to elevate an injured limb, and a safety-net to return for spreading redness, increasing pain, fever, numbness or a cold digit, or a wound that opens. Antibiotics are NOT routine for the clean closed laceration — they are reserved for the bite (amoxicillin-clavulanate), the contaminated laceration in the high-risk host, and the plantar puncture (ciprofloxacin for Pseudomonas), as detailed in the wound assessment topic. Tetanus prophylaxis is decided by wound type and vaccination history and is documented at every closure. Return-to-sport and work advice protects the immature scar for two weeks, with adhesive strips reinforcing the closure over a joint. [1]
Special populations
The child with a laceration is best managed with topical anaesthesia (LET gel), and an absorbable surface suture (Vicryl Rapide) or tissue adhesive to spare the removal visit — the Luck evidence supports absorbable closure on the paediatric face without cosmetic penalty.[2][3] The needle-phobic child with a small low-tension laceration is the ideal tissue-adhesive candidate.[5][9] The elderly patient has fragile, atrophic skin (skin tears) where adhesive strips and tissue adhesive are often kinder than sutures, which tear through the thin dermis. The anticoagulated patient bleeds more from the wound and from the local-anaesthetic injection; meticulous haemostasis and pressure replace dose modification, and a continuous locked suture on the vascular scalp reduces oozing. The cosmetic-site patient with a complex facial laceration (vermillion border, eyelid margin, nasolacrimal apparatus, facial nerve) is referred to plastics for specialist closure — a misaligned vermillion border is visible for life. The diabetic and immunocompromised patient has a lower threshold for delayed closure, antibiotic prophylaxis and a 48-hour review. The pregnant patient is closed with any suture and anaesthetised with lidocaine as for any adult.
Evidence and regional guidelines
The contemporary framework rests on four evidence streams. The material evidence — Luck's randomised trials of absorbable versus non-absorbable sutures on the paediatric face — established that absorbable Vicryl gives cosmetic outcomes equivalent to nylon, sparing the removal visit.[2][3] The tissue-adhesive evidence — Farion's systematic review, the cost-effectiveness trial and the Singer multicentre trial — established equivalence to sutures for the appropriate low-tension wound at lower cost and less pain.[4][8][9] The specific-paediatric-use evidence extends tissue adhesive to tongue, nail-bed and simple paediatric lacerations with cosmetic outcomes equivalent to suture.[5][6][7] The closure-decision evidence — Quinn's study of the contested golden period — reframed closure from a rigid 6-hour clock to an integrated judgement of age, contamination, site and host.[10] The technique-overview evidence — Elfar's 2025 systematic review — summarises the comparative evidence across sutures, adhesives and staples for traumatic ED closure.[1] The Steri-Strip versus subcuticular trial confirms adhesive strips as a needle-free equivalent for the low-tension wound.[11]
ANZ practice note. In Australasian EDs the workhorse skin suture is non-absorbable nylon (Ethilon) or polypropylene (Prolene) on the face and extremities, with absorbable Vicryl for the deep dermal and mucosal layers and Monocryl for subcuticular cosmetic closures. Scalp wounds are stapled whenever speed matters. Tissue adhesive (Histoacryl / Dermabond) and Steri-Strips are first-line for small, low-tension lacerations, especially in children, in line with the Luck and Farion evidence. Removal intervals follow the standard schedule (face 5 days, scalp 7 to 10, body 7 to 10, joints 14). Local anaesthesia uses lidocaine 1 per cent (3 mg/kg plain, 7 mg/kg with adrenaline) and LET gel for paediatric wound anaesthesia. Complex facial lacerations involving the vermillion border, eyelid, lacrimal apparatus or facial nerve are referred to plastics, in line with ACEM guidance that the proceduralist's scope is the straightforward laceration repair. [1]
SAQ — Paediatric facial laceration — suture versus tissue adhesive
10 minutes · 10 marks
A 4-year-old boy presents with a 3 cm clean, non-penetrating laceration on his forehead from a fall 1 hour ago. He is cooperative but anxious. The wound is clean, the edges are well-apposed, and there is no tendon or neurovascular injury.
SAQ — Complex layered closure of a deep, gaping laceration under tension
10 minutes · 10 marks
A 26-year-old man presents with a 6 cm deep laceration on his shin from a kick at football. The wound is gaping and down to the tibialis anterior tendon sheath (tendon intact), with the skin edges retracted by 5 mm. He has no neurovascular or tendon compromise.
Exam pearls
- Suture by site, recite it aloud — 5-0 face, 4-0 body, 3-0 scalp and extremity; non-absorbable nylon/Prolene on the surface, absorbable Vicryl deep and on the paediatric face.
- Evert every bite — perpendicular entry, dermal bite, equal depth; the inverted wound is the commonest cosmetic error.
- Vertical mattress for tension (far-far near-near, perpendicular), horizontal mattress for eversion (parallel to wound) — name the distinction in the OSCE.
- Removal: face 5, scalp 7 to 10, body 7 to 10, joints 14 — the schedule the SCQ tests verbatim.
- Tissue adhesive and Steri-Strips for the small, low-tension, non-moving wound — never on a finger, knee or mucosa; adhesive goes ON the skin, never in the wound bed.
- Absorbable on the paediatric face spares removal without cosmetic cost — the Luck evidence is the answer to the distressed-child OSCE.
- Never close the bite, the puncture, the infected or the heavily contaminated wound — secondary intention; "does closing trap bacteria I cannot irrigate?" is the discriminator.
- Document neurovascular and tendon BEFORE local anaesthesia — the medicolegal step of every repair. [1]
Red flags
[1]References
- [1]Elfar A, Mubarak A, Salem M, Elgamal M. Suture Techniques for Traumatic Wound Closure in the Emergency Department: A Systematic Review of Cosmetic, Functional, and Infection-Related Outcomes Cureus, 2025.PMID 40792329
- [2]Luck R, Tredway T, Gerard J, Eyal D, Krug L, Cunningham J. Comparison of cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations Pediatr Emerg Care, 2013.PMID 23714755
- [3]Luck RP, Tredway T, Gerard J, Eyal D, Krug L, Cunningham J. Cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations Pediatr Emerg Care, 2008.PMID 18347489
- [4]Wong EM, Cheung YF, Hui EP, Chan BD, Lam SH, Lee KH, Chan FK. Cost-effectiveness of Dermabond versus sutures for lacerated wound closure: a randomised controlled trial Hong Kong Med J, 2011.PMID 22147351
- [5]Barton MS, Smith A, O'Brien K, Muzzio C, Bouton K, Kehoe S, Fredette K, Guanche M, Bouton M, Migita R. A Randomized Controlled Comparison of Guardian-Perceived Cosmetic Outcome of Simple Lacerations Repaired With Either Dermabond, Steri-Strips, or Absorbable Sutures Pediatr Emerg Care, 2024.PMID 39141836
- [6]Edwards S, Hitchen S, Ricketts S, Stephenson R, Choudhary S. Is Fixing Pediatric Nail Bed Injuries With Medical Adhesives as Effective as Suturing?: A Review of the Literature Pediatr Emerg Care, 2019.PMID 27977531
- [7]Kazzi MG, Mubarak N, Lutfy R, Kazzi Z. Pediatric tongue laceration repair using 2-octyl cyanoacrylate (dermabond(®)) J Emerg Med, 2013.PMID 23827167
- [8]Singer AJ, Giordano P, Dinulos JG, Mitchell GM, Miller DR, Oetgen SM, Schmitz H, Sohlig K, Sandoval S, Chale S, et al. Evaluation of a novel wound closure device: a multicenter randomized controlled trial Acad Emerg Med, 2011.PMID 21996071
- [9]Farion KJ, Russell KF, Osmond MH, Hartling L, Klassen TP, Powell G, Arbour R, Kennah M, McGahern C, Arora AK, et al. Tissue adhesives for traumatic lacerations: a systematic review of randomized controlled trials Acad Emerg Med, 2003.PMID 12574007
- [10]Quinn JV, Polevoi SK, Kohn MA. Traumatic lacerations: what are the risks for infection and has the 'golden period' of laceration care disappeared? Emerg Med J, 2014.PMID 23314208
- [11]Ladipo-Ajayi OA, Onah II, Arneh EA, Ademola SA, Olawoye OA, Ibrahim B, Adejuyigbe O. Steri-strip(TM) versus subcuticular skin closure of paediatric groin wounds: A randomised study Afr J Paediatr Surg, 2022.PMID 35775513