EM · Plain radiograph interpretation (approach)
X-ray interpretation in the emergency department — the systematic approach
Also known as X-ray interpretation · Plain film interpretation · CXR interpretation · MSK radiograph interpretation
The systematic approach to plain radiography for the emergency medicine trainee — the technical-quality check (projection, penetration, rotation, inspiration), the chest radiograph method (airway, bones, cardiac, diaphragm, effusions, fields, tubes and lines), the musculoskeletal ABCCS method (adequacy and alignment, bones, cartilage and joints, soft tissue, summary), the Salter-Harris paediatric physeal classification, the fracture descriptors (transverse, oblique, spiral, comminuted, buckle, greenstick), the Ottawa ankle and knee rules and the NEXUS and Canadian C-spine rules, and the normal-vs-abnormal-vs-artefact differential. The image-to-action thresholds — free gas under the diaphragm triggering broad-spectrum antibiotics, the misplaced nasogastric tube withdrawn before any feed, hip fracture managed with a fascia-iliaca block. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
5 MCQs with explanations
Target exams
Red flags
Plain radiography is the highest-volume imaging modality in the emergency department. It is fast, cheap, widely available, and low-radiation, and it is the first-line test for the fractured limb, the breathless chest, the swallowed foreign body and the suspected perforation. The Fellowship examiner is not testing whether a candidate can name a favourite film; the test is whether a candidate can apply a reproducible systematic method to any radiograph, in any patient, under pressure, and not miss the tube in the bronchus, the free gas under the diaphragm, or the paediatric growth-plate injury. Pattern recognition fails on the rotated portable film; a system does not. The interpreter — not the radiologist's later report — makes the disposition. [1]

When to use the framework and the principles of a systematic read
Every ED patient with a suspected fracture, a chest symptom or sign, an in-dwelling tube or line, or a suspected bowel obstruction or perforation is interpreted against a plain film. The radiograph is read by the treating clinician at the time of decision — the formal radiologist report is a quality check, not a handover. A scoping review of chest-radiograph interpretation confirms that a structured, checklist-driven read is more reproducible than an unstructured scan, and that the systematic method is teachable.[8] Five principles govern the read. First, assess the technical quality before any pathology — a film that is rotated, under-penetrated or poorly inspired cannot be cleared. Second, use the same ordered sequence every compartment, every time, so nothing is skipped under cognitive load. Third, interpret in parallel with resuscitation — a tension pneumothorax is decompressed, not described. Fourth, read with the clinical question and compare with prior films; a borderline finding that is new is far more significant than one that is chronic. Fifth, state the limitation — a single radiograph excludes almost nothing.
Technical quality — projection, penetration, rotation, inspiration
Before any pathology is sought, the film must pass a quality gate. Projection is named for the direction the beam travels relative to the detector — a PA chest is taken postero-anterior with the beam entering the back, the heart sits close to the detector and is minimally magnified, whereas a portable AP chest magnifies the heart and widens the mediastinum, so the cardiomediastinal contour is never declared abnormal on a single AP film alone. Penetration is adequate when the lower thoracic vertebral bodies are just visible through the cardiac shadow; an under-penetrated film hides the retrocardiac lung and the posterior costophrenic recesses. Rotation is judged from the medial ends of the clavicles, which should sit symmetrically about the spinous process; a rotated chest obliques the hilar contours and distorts the heart, and a rotated c-spine makes the facet joints asymmetric and falsely opens the disc spaces. Inspiration is adequate when five or six anterior ribs intersect the diaphragm, or nine or ten posterior ribs — a poor inspiratory effort crowds the lung bases, elevates the diaphragm, and widens the cardiomediastinal silhouette, simulating disease. [1]
The chest radiograph method — airway to tubes
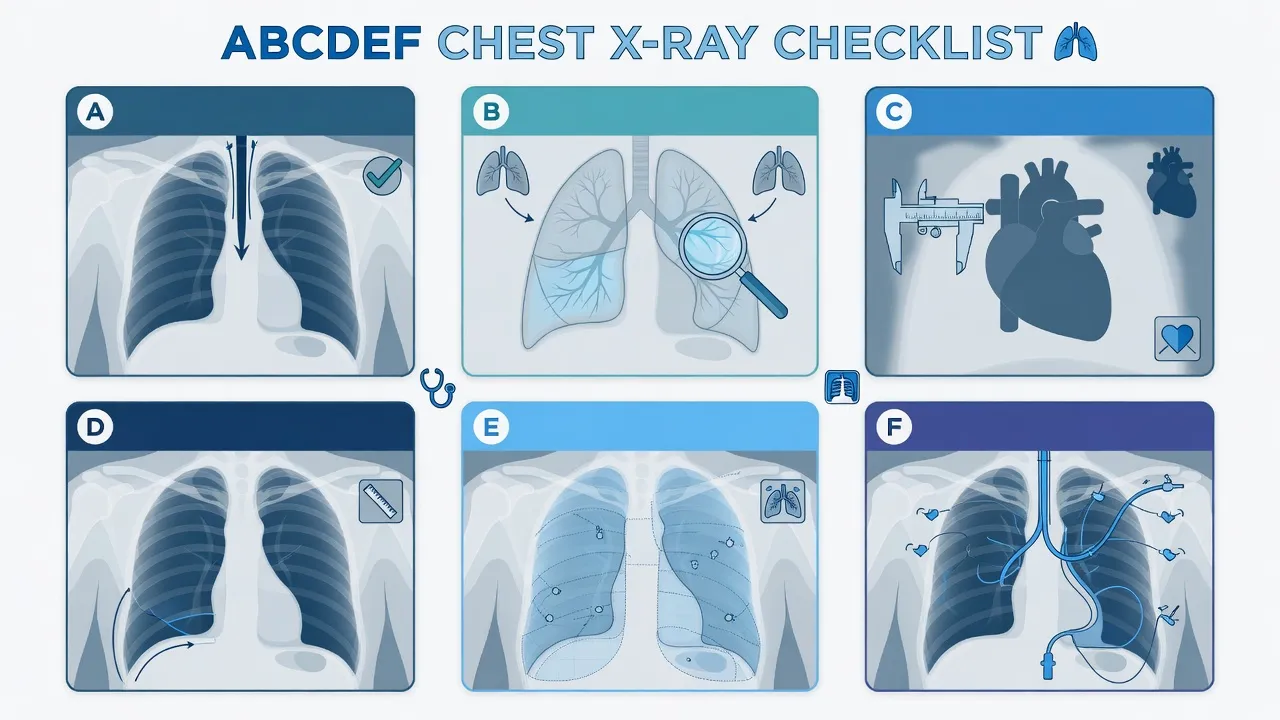
The chest is read in a fixed sequence so that no compartment is missed. The mnemonic encodes the compartments, not the order of importance — the order is the discipline. [1]
The chest radiograph method — the ABCDEFGH sequence
RIP-ABCDE
Projection (PA/AP), penetration, rotation (clavicles symmetric about the spinous process), inspiration (5–6 anterior ribs above the diaphragm)
Name, date, side marker — confirm the film belongs to this patient
Endotracheal tube 2–3 cm above the carina, central line tip in the cavoatrial junction, nasogastric tube not in the bronchus and the tip below the diaphragm, chest drains with the last hole medial to the mid-axillary line
Trachea midline, carina at T4–T5 (the right main bronchus is steeper and shorter — an aspirated or intubated tube preferentially goes right), hila symmetric (the left is up to 1 cm higher)
Trace every rib, the clavicles, the spine and the scapulae — a rib fracture implies transmitted force (flail segment, splenic or hepatic injury)
Cardiothoracic ratio under 0.5 on a PA film, aortic knuckle defined, mediastinum not widened (a widened mediastinum on a trauma AP is non-specific — CT aortogram is the test for dissection)
Right hemidiaphragm up to 3 cm higher than the left, costophrenic angles sharp and deep, free gas sought under the right hemidiaphragm on an erect film
Blunting of a costophrenic angle implies around 200 mL on an erect PA film (lateral detects around 50 mL, decubitus around 5 mL); the meniscus sign; the deep sulcus sign on a supine film is a pneumothorax until proven otherwise
Lung fields compared zone for zone; the silhouette sign (loss of an anatomic border localises the lesion — a left lower zone opacity obliterating the diaphragm is in the lower lobe, one obliterating the heart border is in the lingula); collapse versus consolidation; the minor fissure
The silhouette sign is the single most powerful localiser on a chest radiograph: an opacity that abuts and erases a structure is in contact with it (anterior to the heart border is lingula or middle lobe; the diaphragm is a lower lobe), whereas an opacity that preserves the border lies away from it. Collapse (atelectasis) shows volume loss — shift of the mediastinum or fissure toward the lesion, with crowded vessels — whereas consolidation preserves volume and shows an air bronchogram. [1]
The musculoskeletal method — ABCCS
The limb and joint radiograph is read with a deliberate, layered method that starts with film adequacy and ends with a stated summary. The two-view minimum is non-negotiable — a single anterior-posterior film misses a posterior shoulder dislocation, an undisplaced scaphoid fracture and a subtle radial head fracture. [1]
The musculoskeletal method — ABCCS
ABCCS
Two orthogonal views (AP and lateral, plus oblique for the scaphoid and the elbow); the joint above and below a long-bone fracture; cortical continuity traced; the arcs of Gartland and Shenton (the radial head should line up to the capitellum on every view — if not, a radial head dislocation)
Cortex intact (a break is a fracture); trabecular pattern (disrupted in a subtle impaction; sclerosis or lucency in a stress or pathologic fracture); bone density (osteopenia in the elderly raises the low-energy fracture risk)
Joint space 3–4 mm and symmetrical with the other side (loss is arthropathy — septic, degenerative, inflammatory); congruity of the articular surfaces (a dislocation or subluxation); in the child, the physis is the radiolucent cartilage plate — never mistake a normal physis for a fracture
Swelling, the elbow fat-pad signs, surgical or radio-opaque foreign body, subcutaneous gas (an open fracture or gas-forming infection), the normal psoas shadow lost in a retroperitoneal bleed
State the injury in plain language (bone, site, pattern, displacement, open or closed, intra- or extra-articular, Salter-Harris grade if a child) and the next step — the read triggers an action, not a label
Salter-Harris — the paediatric physeal classification
The growing long bone has a radiolucent cartilage growth plate (the physis) between the epiphysis (the secondary ossification centre at the joint end) and the metaphysis (the flared end of the shaft). A fracture that crosses the physis can arrest growth, and the Salter-Harris grade predicts that risk — higher grades carry a higher rate of premature physeal closure and growth disturbance.[7]
The Salter-Harris grades (SALTR mnemonic)
The paediatric skeleton also produces patterns that have no adult equivalent. A buckle (torus) fracture is a compression failure — the cortex buckles and impinges but does not break through; the distal radius after a fall onto the outstretched hand is the archetype, managed in a removable splint. A greenstick fracture breaks one cortex and leaves the opposite intact (incomplete, plastic paediatric bone). A plastic (bowing) deformation bows a long bone without a discrete fracture line. An avulsion fractures a fragment at a tendon or ligament insertion — the tibial spine (anterior cruciate ligament), the patellar sleeve (quadriceps), the medial epicondyle of the elbow — and is the sports-injury archetype in adolescents. [1]
Fracture descriptors — the language of the read
The summary step requires the fracture to be described in the standard language. A transverse fracture is perpendicular to the long axis (a direct blow, stable); an oblique runs at an angle (a mix of compression and bending); a spiral winds around the shaft (a torsion mechanism — in a non-ambulant child, a spiral long-bone fracture is a non-accidental injury red flag). A comminuted fracture produces more than two fragments; a segmental fracture produces a separate shaft fragment between two fracture lines (a high-energy open-injury pattern); a butterfly fragment is a triangular wedge torn off by bending. A fracture is open (compound) when the wound communicates with the outside — antibiotics and tetanus cover are mandatory. A pathologic fracture traverses abnormal bone (metastasis, myeloma, a simple bone cyst). [1]
Differential diagnosis — normal, abnormal, artefact
A radiograph is a two-dimensional shadow of a three-dimensional patient, and the eye is fooled. Every film is judged against four possibilities. [1]
Normal variant
- Accessory ossicles (os trigonum at the posterior talus, os subfibulare, bipartite patella, os vesalianum) — smooth, well-corticated margins distinguish them from a fresh fragment
- A sesamoid bone at the first metatarsophalangeal joint, a strutted vertebral body, a bifid rib — developmental, not traumatic
- A developing secondary ossification centre in a child — compare with the contralateral side if uncertain
- Manage as normal; document for the record so it is not re-flagged as a fracture
Acute pathology
- A sharp, non-corticated fracture line; soft-tissue swelling; a joint effusion or fat-pad sign; cortical step
- An acute lung opacity with an air bronchogram (consolidation); a pleural meniscus (effusion); a pneumothorax with absent lung markings beyond a pleural line
- Free gas under the diaphragm; dilated loops of bowel with valvulae conniventes (small bowel) or haustra (large bowel)
- Manage to the clinical picture — the radiograph confirms and localises
Chronic / healed
- A healed fracture with callus is sclerotic and bridging; an old compression fracture of a vertebral body is wedge-shaped with preserved cortex
- Chronic obstructive lung disease (hyperinflation, flat diaphragms, barrel chest) and old apical fibrosis (tuberculosis)
- Compare with prior films — a chronic finding does not explain an acute presentation on its own
- Document and do not over-investigate
Artefact
- A skin fold produces a dark line with normal vascular markings seen beyond it (a true pneumothorax has an actual pleural line and absent markings beyond)
- Motion unsharpness blurs the cortical margin and the trabeculae; grid lines and jewellery cast shadows
- An external foreign body (button, ECG dot, hair braid) projects over the lung fields
- Repeat or cross-section if uncertain and the patient is stable
The decision rules — when to image in the first place
The decision to image is itself an examinable skill, and the high-yield rules were derived and validated to reduce unnecessary radiography without missing injury. [1]
The validated imaging decision rules
The Ottawa ankle rule has a sensitivity approaching 100% and a near-perfect negative predictive value for clinically significant malleolar fracture, reducing ankle radiography by around a third without a missed injury.[1] The Ottawa knee rule shares the same near-perfect sensitivity for clinically significant knee fracture.[2] The Pittsburgh rule performs comparably and is a recognised alternative.[3] For the cervical spine, NEXUS requires all five low-risk criteria to be met before imaging is withheld (sensitivity 99.6% for clinically important injury)[4] and the Canadian C-spine rule, which is more sensitive and more specific, applies to alert and stable trauma patients.[5]
Image-to-action management thresholds
The interpretation does not stop at a label — several findings immediately trigger a drug, a procedure or a referral. The doses are committed to memory because the unstable patient cannot wait for a lookup. [1]
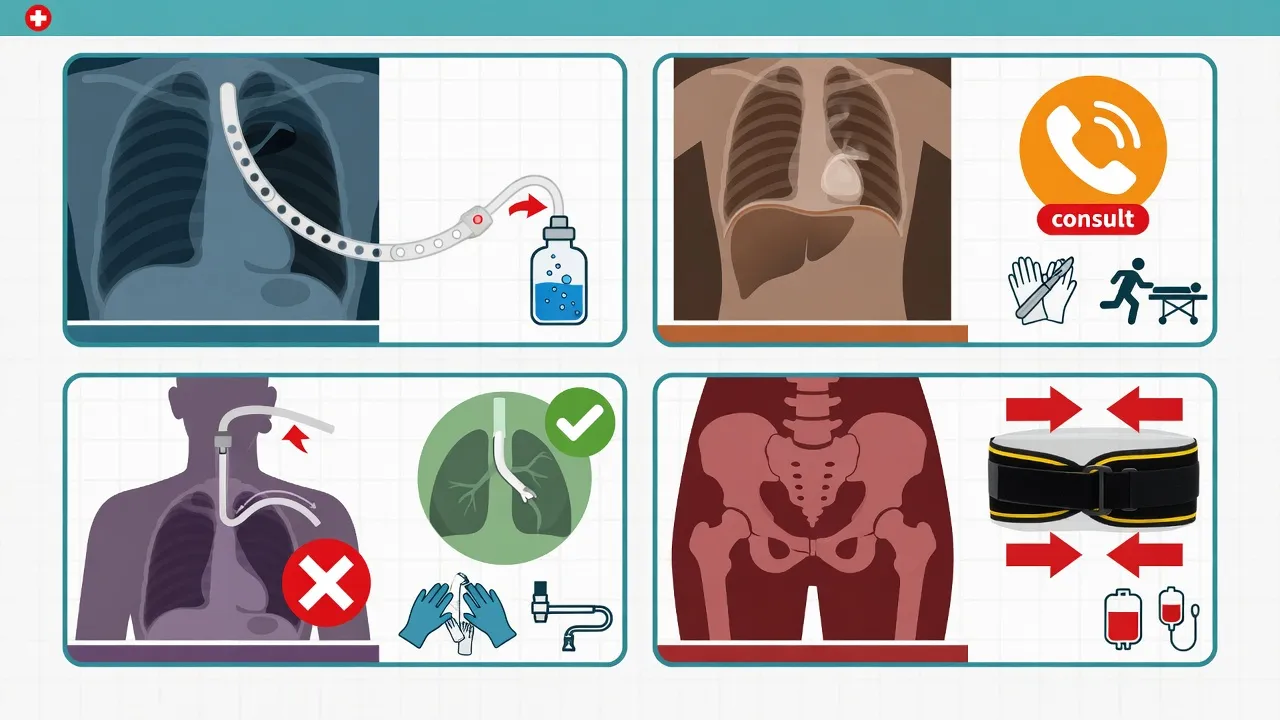
Tubes, lines and the portable trauma film
The intubated trauma patient is radiographed portably, supine and AP, which magnifies the heart and widens the mediastinum — a widened mediastinum on an AP trauma film is a prompt to a CT aortogram, not a diagnosis of dissection. The endotracheal tube tip should sit 2 to 3 cm above the carina (around the T4–T5 level); too high risks extubation with neck movement, too low risks main-stem intubation (the right main bronchus is steeper, shorter and more vertical, so a tube advanced too far goes right). The central venous catheter tip should lie in the cavoatrial junction, below the inferior border of the right main bronchus and above the right atrium, and not curl in the internal jugular or the contralateral subclavian. The nasogastric tube must not coil in the oropharynx and the tip must lie below the diaphragm in the stomach — a tube in a main bronchus is a never-event, withdrawn before any use. [1]
Special populations
The paediatric skeleton has open physes (Salter-Harris applies), accessory ossicles that mimic fracture, and plastic/bowing and greenstick patterns; the non-accidental-injury patterns are examinable — a posterior rib fracture near the costovertebral junction, a corner (bucket-handle) fracture of a long-bone metaphysis, a spiral long-bone fracture in a non-ambulant child, and multiple fractures of differing ages. The elderly patient has osteopenia, so a low-energy mechanism (a fall from standing) produces a hip, a distal radius, a proximal humerus or a vertebral compression fracture, and a normal radiograph in osteopenic bone does not exclude an occult fracture — an early MRI is the test. The pregnant patient is imaged under the ALARA principle; a single chest radiograph delivers around 0.01 millisieverts, far below the deterministic threshold for fetal harm at 100 millisieverts, and is justified when clinically indicated, with the abdomen shielded. The intubated and ventilated patient is radiographed portably AP and supine, with a magnified mediastinum and pooled posterior fluid — free intraperitoneal gas is sought on a supine film by the Rigler sign (gas on both sides of the bowel wall) or the football sign. [1]
Common errors and pitfalls
The recurring errors are reading only one view (the missed scaphoid, the missed posterior shoulder dislocation); the satisfaction of search — a second abnormality is missed once the first is found; declaring a widened mediastinum abnormal on a single rotated AP trauma film; clearing a cervical spine on an inadequate film (the C7–T1 junction must be visible); missing the nasogastric tube in the bronchus; mistaking a skin fold for a pneumothorax (the deep sulcus sign on a supine film is a true tension pneumothorax until proven otherwise); accepting a radiologist report in lieu of the clinician's own read; and forgetting that a negative radiograph excludes almost nothing — the early scaphoid fracture is occult for up to two weeks, early osteomyelitis is occult, and a pulmonary embolism produces a normal chest radiograph more often than an abnormal one. [1]
Evidence and regional guidelines
The imaging decision rules are among the most validated instruments in emergency medicine: the Ottawa ankle and knee rules have near-perfect sensitivity and have safely reduced radiography worldwide,[1][2] with the Pittsburgh knee rule as a comparable alternative.[3] The NEXUS and Canadian C-spine rules together define the cervical-spine imaging gate.[4][5] For paediatric elbow injury, the radiographic fat-pad sign is a high-yield occult-fracture marker — a meta-analysis of children with a positive posterior fat pad and no visible fracture line found an occult fracture in around three quarters, supporting immobilisation and follow-up.[6] Salter-Harris grades IV and V carry the highest premature-physeal-closure risk and warrant orthopaedic follow-up.[7] Structured, checklist-based chest-radiograph interpretation improves reproducibility and is teachable.[8] The systematic method, the Salter-Harris classification and the decision-rule thresholds are global and are consistent across the ACEM, ATLS, Royal College of Radiologists and ACR frameworks; the local protocol governs the trauma CT-first pathway and the procedural-sedation service.
ANZ practice note. The systematic plain-film read follows the ACEM and Royal Australian and New Zealand College of Radiologists (RANZCR) guidance, with major trauma imaged by whole-body CT first (the adult c-spine is cleared by CT, not plain film). The Ottawa ankle and knee rules are standard ED practice; the NEXUS and Canadian C-spine rules govern cervical-spine imaging. Procedural sedation (ketamine 1 to 1.5 mg per kilogram intravenously) follows the ANZCA/ACEM joint guidance and is delivered by a credentialed sedationist. The pregnant patient is imaged under the ARPANSA Code of Practice and the ALARA principle — a single diagnostic chest radiograph is justified and the fetus is shielded. [1]
The chest radiograph — the ABCDE method in detail
The ABCDE method is the workhorse chest-radiograph sequence used in every ED and ICU round. It encodes the same compartments as the longer RIP-ABCDEFGH sequence but is the version most examinable at the viva, because it is rapid, reproducible and exhaustive in five letters. Every letter is read in turn, and no compartment is skipped.[8]
The chest radiograph — ABCDE
ABCDE
The trachea lies midline — deviation suggests a tension pneumothorax (pushed away from the side), lobar collapse (pulled toward the side) or a large effusion or thyroid mass (pushed). The carina sits at T4–T5; the right main bronchus is steeper, shorter and more vertical, so an aspirated foreign body or an over-advanced endotracheal tube goes right. The hila are symmetric, with the left up to 1 cm higher than the right; a unilateral hilar enlargement raises a tumour, a node or a pulmonary artery
Trace every rib (a posterior rib fracture near the costovertebral junction is a non-accidental-injury marker in children), both clavicles, the spine and the scapulae. Look for a lytic lesion (myeloma, metastasis, brown tumour of hyperparathyroidism), a sclerotic lesion (healed fracture, osteoblastic metastasis from prostate or breast, Paget disease), a cortical break (rib, clavicle) and the subcutaneous emphysema of a pneumothorax or pneumomediastinum
The cardiothoracic ratio is measured on a PA film — greater than 0.5 (the cardiac width exceeds half the thoracic width) is cardiomegaly. On a portable AP film the heart is magnified, so cardiomegaly is never declared on a single AP view. The aortic knuckle should be crisp; a blurred or lost aortic knuckle with a left lower zone opacity is a haemothorax or a descending thoracic aortic aneurysm. A widened mediastinum (>8 cm at the aortic knuckle on a trauma AP) is a dissection until a CT aortogram excludes it
The right hemidiaphragm sits up to 3 cm higher than the left (the liver). The costophrenic angles are sharp and deep — blunting implies a pleural effusion (around 200 mL on an erect PA film; 50 mL on a lateral; 5 mL on a decubitus). Free gas under the right hemidiaphragm on an erect film is a perforated viscus; under the left it is harder (the gastric fundus) but the Rigler double-wall sign on a supine film confirms it. A raised hemidiaphragm alone suggests phrenic nerve palsy, a subpulmonic effusion or lobar collapse
The costophrenic angles and apices for a meniscus effusion and an apical cap; the extrathoracic soft tissues for surgical emphysema, breast shadows and the supraclavicular fossae for a mass. On a supine trauma film the deep sulcus sign (a deep, lucent costophrenic angle) is a pneumothorax until proven otherwise — and with hypotension and tracheal deviation it is a tension pneumothorax
Common ED chest radiograph findings — a pattern library
The Fellowship candidate is expected to recognise the high-yield chest-radiograph patterns at the bedside and state the disposition. The patterns below are the recurring presentations of the breathless, the febrile and the shocked ED patient. [1]
Pneumothorax
- A visceral pleural line with absent lung markings beyond it — the defining finding
- The apices are checked first on an erect film (air rises); the costophrenic angle and the deep sulcus on a supine film
- A skin fold mimics it but has normal vascular markings beyond the line; a true pneumothorax has none
- Tension features — tracheal deviation AWAY from the side, mediastinal shift, flattened ipsilateral hemidiaphragm, hyperlucent hyperexpanded hemithorax — mandate immediate needle decompression (2nd intercostal space mid-clavicular line, or 5th intercostal space mid-axillary line) before any imaging
Pneumonia (consolidation)
- A fluffy airspace opacity with an air bronchogram (the bronchi are seen as dark branching tubes through the white alveolar exudate) — the hallmark of consolidation
- Volume is preserved (unlike collapse); the silhouette sign localises it — opacity obliterating the right heart border is right middle lobe, the diaphragm is lower lobe, the left heart border is lingula
- An associated pleural effusion (para-pneumonic) raises an empyema; a cavity raises a lung abscess or a necrotising pneumonia
- Manage with culture-directed antibiotics, oxygen and the sepsis bundle; reassess at 48–72 hours — failure to improve warrants a CT and a resistant-organism or complication search
Pulmonary oedema
- The classic bat-wing or butterfly perihilar alveolar opacities of acute cardiogenic pulmonary oedema
- Kerley B lines — short horizontal linear opacities at the lung bases abutting the pleura — represent interlobular septal thickening from interstitial fluid
- Cardiomegaly, upper-lobe venous diversion (the upper-lobe vessels larger than the lower), pleural effusions (usually right-sided first) and pulmonary arterial enlargement complete the congestive heart failure picture
- Manage with oxygen, nitrates and high-dose loop diuretic; NIV (CPAP 5–10 cm) for the failing patient — the nitrate does the heavy lifting in the hypertensive pulmonary oedema
Lung mass / nodule
- A discrete solitary pulmonary nodule or mass — spiculated, irregular margins favour malignancy; smooth, well-circumscribed favour a benign lesion (hamartoma, granuloma)
- Calcification (central, laminated or popcorn) favours benignity; upper-lobe location and cavitation favour tuberculosis or squamous carcinoma
- A hilar mass with lobar collapse is the classic bronchogenic carcinoma with post-obstructive pneumonitis (the golden S sign of Golden in a right upper lobe collapse)
- Every incidental pulmonary nodule follows a validated follow-up protocol (Fleischner or Lung-RADS) — discharge is never on a single film
Pneumoperitoneum
- Free intra-abdominal gas, seen as a crescent of lucency beneath the right hemidiaphragm on an erect chest film — the single most sensitive plain-film sign of a perforated viscus
- On a supine film look for the Rigler double-wall sign (gas outlining both sides of the bowel wall), the football sign (a large lucent abdomen) or the outline of the falciform ligament
- A perforated peptic ulcer gives a large volume of free gas; a lower-GI perforation (diverticulum, appendix, colon) gives less; a closed perforation with a walled-off abscess may show none
- A perforation is a surgical emergency — antibiotics (piperacillin-tazobactam 4.5 g IV) and an urgent surgical and gastroenterology referral; the volume of free gas correlates with the severity of the underlying perforation
The abdominal radiograph — the systematic approach
The plain abdominal radiograph (AXR) is a low-yield, high-overuse investigation. Its evidence-based indications are narrow — the suspected bowel obstruction, the perforation (an erect chest film is better), the radiopaque foreign body or ingested packet, and the assessment of an indwelling tube or stent. A systematic read prevents the common error of declaring a non-obstructive film obstructive because of normal calibre bowel gas. [1]
The systematic abdominal radiograph read
Confirm adequacy and the clinical question
Identify the bowel gas pattern — small versus large bowel
Measure the calibre and look for the obstruction
Search for the surgical emergencies
Assess the calcifications and the bones
State the summary and the disposition
Small bowel
- Central location in the abdomen
- Valvulae conniventes (plicae circulares) — COMPLETE mucosal folds crossing the full lumen at close regular intervals (every 2–3 cm)
- Calibre up to 2.5–3 cm; a feathrous mucosal pattern in the jejunum, a featureless ileum
- No solid faecal material; contains only gas and fluid
- Dilated small bowel over 3 cm in a step-ladder with air–fluid levels = small-bowel obstruction
Large bowel
- Peripheral location — frames the abdomen
- Haustra — INCOMPLETE folds that do not cross the full lumen, at wider irregular intervals
- Calibre up to 5–6 cm (the caecum up to 9 cm before the perforation risk)
- May contain solid faecal material with a mottled gas pattern
- Dilated large bowel over 6 cm with a distal cut-off = large-bowel obstruction
The pelvic radiograph — fractures and the hip
The single AP pelvic radiograph is part of the ATLS primary survey of the major-trauma patient and answers two questions in seconds: is there a mechanically unstable pelvic ring injury, and is there a proximal femoral or acetabular fracture? A systematic read of the rings, the arcs and the hip joints prevents the missed sacral impaction fracture and the subtle pubic rami fracture in the elderly faller. [1]
The systematic pelvic radiograph read
The three pelvic rings
The pubic rami and the symphysis
The sacrum and the sacro-iliac joints
The acetabulum and the hip
The femur and the soft tissues
The cervical spine lateral radiograph — the ABCS method
The lateral cervical spine film was once the cornerstone of the trauma clearance; in modern major-trauma practice the adult cervical spine is cleared by CT. The lateral c-spine film remains high-yield exam material and is still used where CT is unavailable or in the paediatric and low-risk patient. The ABCS method — adequacy, bones, cartilage, soft tissue — is the systematic read. [1]
The cervical spine — ABCS lateral read
ABCS
Adequate only if the C7–T1 junction is visible (a swimmer view or CT if not). Trace the four lordotic curves — the anterior longitudinal ligament line along the anterior vertebral bodies, the posterior longitudinal ligament line, the spinolaminal line (the posterior border of the spinal canal), and the tips of the spinous processes. All four should be smooth and continuous; any step is a subluxation or a dislocation. The predental space (the atlanto-dental interval between the anterior arch of C1 and the dens) is under 3 mm in the adult and under 5 mm in the child — widening is a transverse ligament rupture (rheumatoid, trauma, Down syndrome)
Check every vertebral body for height (a wedge or compression fracture), the dens for a type I, II or III fracture (the Anderson and DAlonzo classification), the pedicles, the facet joints and the spinous processes (a clay-shovellers fracture of C7 or T1 is an avulsion of the spinous process by the supraspinous ligament). A teardrop fracture — a small antero-inferior fragment with posterior subluxation — is a devastating flexion injury with an anterior cord syndrome
The disc spaces should be uniform and symmetric; a narrowed disc space is a degenerative disc disease or, with a step in the lines, a traumatic disc injury. The facet joints should overlap in a shingled pattern; a jumped or locked facet (the superior facet displaced over the inferior) is a hyperflexion injury — bilateral locked facets are unstable and carry a high cord-injury rate
The prevertebral soft-tissue stripe is measured at C3–C4 (under 7 mm, or under a third of the vertebral body width) and below C4 (under 22 mm, or under the vertebral body width). Widening is a retropharyngeal haematoma from an anterior cervical spine injury — and may be the ONLY sign of an unstable injury on a normal-appearing film. The airway should be midline; the tracheal and the endotracheal tube positions are confirmed
High-yield trial evidence — the validated imaging decision rules
The imaging decision rules are among the most rigorously validated instruments in all of medicine, and the Fellowship candidate is expected to know the rule, the trial that derived it, and the operating characteristics. The Ottawa ankle rule, the Ottawa and Pittsburgh knee rules, the NEXUS and Canadian C-spine rules, and the paediatric fat-pad meta-analysis are the irreducible minimum.[1][2][3][4][5][6]
Stiell 1995 (BMJ) — the Ottawa ankle rule
BMJ
PMID 7663253
Key finding
A multicentre implementation trial introducing the Ottawa ankle rule as the imaging gate for the acute ankle injury — bone tenderness over the posterior edge or tip of either malleolus, the navicular or the base of the fifth metatarsal, OR inability to bear weight four steps in the ED or at the time of injury. The rule has a sensitivity approaching 100 per cent and a near-perfect negative predictive value for clinically significant malleolar fracture, and reduced ankle radiography by around a third without a missed injury.
Practice change
The Ottawa ankle rule is the most validated imaging decision rule in emergency medicine and the default imaging gate for the acute ankle and midfoot injury worldwide; a patient meeting no criterion is discharged without a radiograph and with safety-net advice.
Stiell 1996 (JAMA) — the Ottawa knee rule
JAMA
PMID 8594242
Key finding
A prospective validation of a knee-radiography decision rule — age 55 or over, isolated patella tenderness, inability to flex the knee to 90 degrees, or inability to bear weight four steps — with a sensitivity near 99 per cent for clinically significant knee fracture.
Practice change
The Ottawa knee rule is the standard imaging gate for the acute knee injury; the patient meeting no criterion is cleared without a radiograph. The rule halves unnecessary knee films.
Seaberg 1998 (Ann Emerg Med) — the Pittsburgh knee rule
Annals of Emergency Medicine
PMID 9656942
Key finding
A multicentre comparison of two clinical decision rules for knee radiography. The Pittsburgh knee rule — blunt trauma or a fall, AND age under 12 or over 50, OR inability to walk four full weight-bearing steps in the ED — performed with comparable sensitivity and specificity to the Ottawa knee rule.
Practice change
The Pittsburgh knee rule is a recognised alternative imaging gate; either rule may be used, but the two are not applied together. The Pittsburgh rule is the natural choice in the paediatric and the older patient.
Hoffman 2000 (NEJM) — the NEXUS cervical-spine rule
New England Journal of Medicine
PMID 10891516
Key finding
A prospective multicentre study of over 34 000 blunt-trauma patients validating the five NEXUS low-risk criteria — no midline cervical tenderness, no focal neurological deficit, a normal level of alertness, no intoxication, and no painful distracting injury. With all five criteria present the rule had a sensitivity of 99.6 per cent and a negative predictive value of 99.9 per cent for clinically important cervical-spine injury.
Practice change
NEXUS is the foundational cervical-spine imaging gate — if all five criteria are present the cervical spine is cleared clinically without imaging. The Canadian C-spine rule is the more sensitive and more specific alternative where it can be applied.
Stiell 2001 (JAMA) — the Canadian C-spine rule
JAMA
PMID 11597285
Key finding
A prospective multicentre derivation and validation of the Canadian C-spine rule for alert and stable trauma patients (Glasgow Coma Scale 15, stable vital signs). Three high-risk factors (age over 65, a dangerous mechanism, paraesthesia in the extremities) mandate imaging; six low-risk factors (a simple rear-end motor-vehicle collision, sitting up in the ED, ambulatory at any time, delayed onset of neck pain, absence of midline tenderness — and the ability to rotate the neck 45 degrees left and right) allow safe clearance without imaging. Sensitivity approached 100 per cent and exceeded NEXUS in both sensitivity and specificity.
Practice change
The Canadian C-spine rule is the preferred cervical-spine imaging gate for the alert and stable trauma patient — it is more sensitive and more specific than NEXUS and reduces imaging further, but applies only when the patient is alert and stable.
Kappelhof 2022 (JBJS Reviews) — the elbow fat-pad sign and occult fractures (meta-analysis)
JBJS Reviews
PMID 36326720
Key finding
A meta-analysis of children presenting with a radiographic fat-pad sign of the elbow and no visible fracture line on the index film. A posterior fat pad was associated with an occult intra-articular fracture in around three quarters of the children; the posterior fat pad is never a normal finding, whereas a sail-sign anterior fat pad alone may be.
Practice change
A positive posterior fat-pad sign on a paediatric elbow radiograph is treated as an occult fracture until proven otherwise — immobilise and bring the child back for repeat imaging or an early MRI; the absence of a visible fracture line does not exclude injury.
Additional chest radiograph pearls — the bedside signs
The high-yield signs below are the recurring discriminating findings on the ED chest film. Each converts a descriptive read into a disposition in seconds — the deep sulcus sign to a decompression, the football sign to a laparotomy, the golden S sign to a bronchoscopy. [1]
[1] [1] [1] [1] [1] [1] [1] [1]Additional comparison tables — the discriminating read
Cardiogenic pulmonary oedema
- Perihilar (bat-wing or butterfly) alveolar opacities that are symmetric and fluffy
- Kerley B lines — interlobular septal thickening from interstitial fluid at the lung bases
- Cardiomegaly (CTR over 0.5 on a PA film), upper-lobe venous diversion (the upper-lobe vessels larger than the lower), pulmonary arterial enlargement
- A pleural effusion, usually right-sided first; the patient is hypertensive, cold, and clammy with a third heart sound
- Resolves rapidly with oxygen, high-dose loop diuretic and nitrate; CPAP 5 to 10 cm for the failing patient — the nitrate does the heavy lifting in the hypertensive pulmonary oedema
- Cephalisation, then interstitial (Kerley), then alveolar (bat-wing) — the three radiographic stages track the rising wedge pressure
Non-cardiogenic (ARDS)
- Diffuse, bilateral, patchy alveolar opacities that are often peripheral and posterior — NOT confined to the hilum
- NO cardiomegaly, NO upper-lobe venous diversion, NO Kerley B lines, NO pleural effusion in the early phase — the heart is normal
- Air bronchograms are prominent (the alveoli fill but the airways stay open); the opacities appear over 24 to 72 hours
- The patient is normotensive or hypotensive, warm, and vasodilated; a clear precipitant (sepsis, aspiration, trauma, pancreatitis) within the week
- Does NOT resolve with diuretic — the opacities persist and the hypoxaemia is severe and refractory (a PaO₂/FiO₂ under 300 defines ARDS by the Berlin definition)
- Lung-protective ventilation (6 mL/kg ideal body weight, plateau pressure under 30) and prone positioning for the severe case
PA chest film (departmental)
- Beam enters the back, exits the front; the heart is close to the detector and minimally magnified
- Cardiothoracic ratio can be measured — over 0.5 is cardiomegaly
- Full inspiratory effort — 5 to 6 anterior ribs or 9 to 10 posterior ribs above the diaphragm
- Standard 6-foot (1.8 m) tube-to-film distance minimises geometric magnification
- The projection on which the cardiomediastinal contour and the mediastinal width are declared
- Obtained erect, patient cooperative — not available for the ventilated, the supine, or the trauma patient
AP chest film (portable / trauma)
- Beam enters the front, exits the back; the heart is further from the detector and magnified
- Cardiothoracic ratio CANNOT be measured — cardiomegaly is never declared on a single AP film
- Often a poorer inspiratory effort (fewer ribs), crowding the lung bases and elevating the diaphragm
- Shorter tube-to-film distance (around 1 m) increases geometric magnification of all central structures
- The mediastinum is widened and the heart is enlarged — a non-specific finding that prompts a PA film or a CT rather than a label
- The standard film for the intubated, the ITU, and the supine trauma patient; rotation and penetration are the additional quality issues
Small bowel obstruction
- Dilated central small-bowel loops over 3 cm in a step-ladder pattern
- Prominent valvulae conniventes (complete mucosal folds crossing the full lumen every 2 to 3 cm)
- Air–fluid levels on an erect film, in a step-ladder or the string-of-beads pattern on a supine film
- A paucity of colonic and rectal gas (the distal bowel is decompressed) — the key discriminating feature from a paralytic ileus
- The commonest cause in the virgin abdomen is an adhesion; with a surgical scar, an internal hernia, a malignancy or a volvulus
- Manage with nasogastric decompression, intravenous fluids, and an early surgical review — a closed-loop or a strangulated obstruction is an emergency
Paralytic ileus / pseudo-obstruction
- Diffuse, uniform gaseous dilatation of BOTH the small bowel and the large bowel, including the rectum
- No mechanical cut-off point, no discrete transition zone — the gas is distributed throughout
- Air–fluid levels may be present but are not in a step-ladder pattern; the bowel is not disproportionately dilated in one segment
- The rectum and the sigmoid contain gas (the distinguishing feature — gas throughout, no distal decompression)
- Causes: post-operative, electrolyte disturbance (hypokalaemia), opioids, sepsis, retroperitoneal haemorrhage, diabetic autonomic neuropathy
- Manage the cause (correct the potassium, stop the opioid, treat the sepsis); nasogastric decompression and electrolyte correction usually resolve it; a pseudo-obstruction (Ogilvie syndrome) may need neostigmine or colonoscopic decompression
The tube-and-line check — the portable film that saves or kills
Every portable chest film on an intubated or line-bearing patient includes a mandatory line check before the lung fields are read — the tube in the bronchus is the never-event that the radiograph is there to catch. A structured check prevents the misplaced feed, the pneumothorax from a central line, and the over-advanced endotracheal tube. [1]
The structured tube-and-line check on every portable chest film
Endotracheal tube
Central venous catheter
Nasogastric tube
Chest drain and the pleural tubes
Pacing wire, surgical hardware and the lines summary
Additional exam pearls — the plain-film viva
[1]SAQ — The supine chest radiograph in the multi-trauma patient
10 minutes · 10 marks
A 24-year-old man involved in a high-speed motor vehicle collision is intubated in the ED. A portable supine AP chest radiograph is performed as part of the primary survey. The patient has received 2 units of blood via a right internal jugular central line.
SAQ — The lateral cervical spine radiograph in the trauma patient
10 minutes · 10 marks
A 70-year-old woman is brought to the ED after a fall from standing. She complains of neck pain. GCS 15, no neurological deficit. A lateral cervical spine radiograph is performed as the initial imaging.
Exam pearls
- Read every film in the same sequence — quality, then compartments, then state the finding and the next action. The method is the mark, not the one-liner.
- ABCCS for the limb: adequacy and alignment, bones, cartilage and joints, soft tissue, summary. The two-view minimum is non-negotiable; a single AP film misses the posterior dislocation and the scaphoid.
- Salter-Harris SALTR: I slipped, II above, III lower, IV through all, V rammed. Grades IV and V carry the growth-arrest risk and need orthopaedic follow-up.
- The posterior fat pad is always abnormal — an occult intra-articular elbow fracture in around three quarters of children, even when no line is seen.
- The silhouette sign localises the pathology — an opacity that erases the heart border is lingula or middle lobe; one that erases the diaphragm is lower lobe.
- A skin fold has normal lung markings beyond it; a true pneumothorax does not. The deep sulcus sign on a supine film is a tension pneumothorax until proven otherwise.
- Tubes and lines are part of every chest radiograph — endotracheal tube 2 to 3 cm above the carina, central line tip in the cavoatrial junction, nasogastric tube not in a bronchus.
- A normal radiograph excludes almost nothing — immobilise the suspicious scaphoid and repeat at 7 to 14 days or CT it. [1]
Red flags
[1]References
- [1]Stiell IG, McKnight RD, Greenberg GH, et al. Multicentre trial to introduce the Ottawa ankle rules for use of radiography in acute ankle injuries. Multicentre Ankle Rule Study Group BMJ, 1995.PMID 7663253
- [2]Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries JAMA, 1996.PMID 8594242
- [3]Seaberg DC, Jackson R Multicenter comparison of two clinical decision rules for the use of radiography in acute, high-risk knee injuries Ann Emerg Med, 1998.PMID 9656942
- [4]Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group N Engl J Med, 2000.PMID 10891516
- [5]Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients JAMA, 2001.PMID 11597285
- [6]Kappelhof B, Hageman S, Bramer WM, et al. Occult Fractures in Children with a Radiographic Fat Pad Sign of the Elbow: A Meta-Analysis of 10 Published Studies JBJS Rev, 2022.PMID 36326720
- [7]Roth OS, Schleich CLA, Wessels C, et al. Risk Factors and Surgical Sequelae of Physeal Arrest in Pediatric Salter-Harris III and IV Medial Malleolus Fractures J Pediatr Orthop, 2026.PMID 41230683
- [8]Sethole KM, dela Cruz FVR, Adeyomolu MA Checklists for interpreting chest radiographs: a scoping review protocol Syst Rev, 2023.PMID 37649115
- [9]Abosayed AK, Salim A, Hadid AM Prognostic value of free air under diaphragm on chest radiographs in correlation with peritoneal soiling intraoperatively Emerg Radiol, 2023.PMID 36515771