Paeds · mental-behavioural-and-psychosomatic
Psychopharmacology and psychotropic medicines in children and adolescents
Also known as Paediatric psychopharmacology · Psychotropic medicines in children · Child and adolescent psychiatric medication · ADHD medication · Paediatric antidepressant prescribing · Antipsychotic use in youth
Fellowship guide to psychopharmacology in children and adolescents: developmental pharmacokinetics, the major drug classes (stimulants, non-stimulants, SSRIs, antipsychotics, mood stabilisers, melatonin), starting-dose and titration frameworks, the FDA black-box suicidality warning, antipsychotic metabolic monitoring, valproate teratogenicity, choice by indication and age with trial evidence, adverse effects, and exam pearls across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 10-year-old who has just been started on methylphenidate and is suddenly eating almost nothing at lunch, a 15-year-old three weeks into fluoxetine who tells you she feels "wired and worse," and a 7-year-old with autism on risperidone whose weight has jumped two centiles in six months. Those three vignettes are the heart of paediatric psychopharmacology: the same drug that helps can also change appetite, mood, growth and metabolism in a developing child, and the clinician's job is to anticipate, detect and weigh that balance. [12] [21]
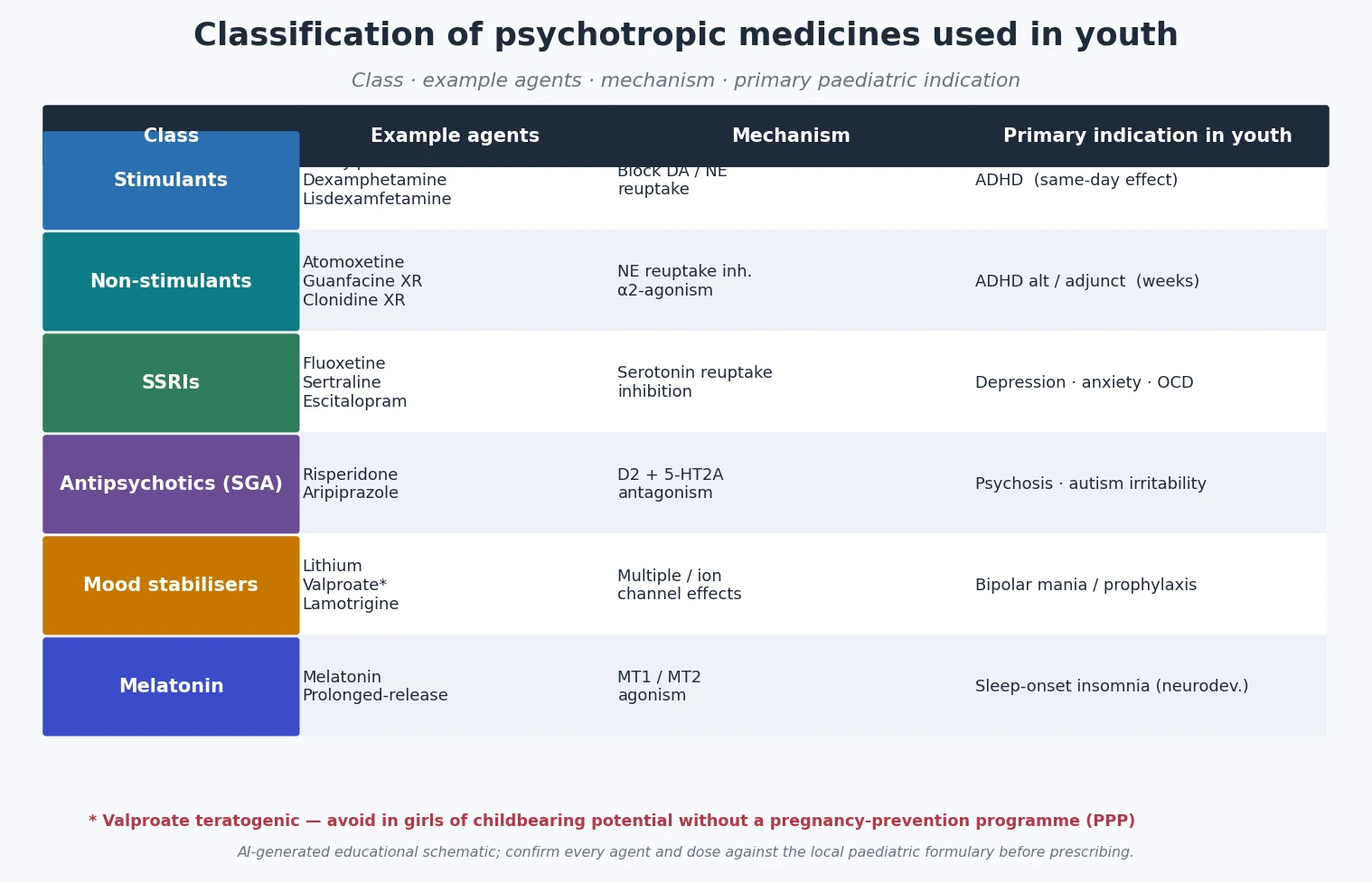
A psychotropic medicine is any drug that acts on the central nervous system to change mood, behaviour, cognition, arousal or sleep. In children and adolescents the practical classes are stimulants and non-stimulants (for ADHD), antidepressants (chiefly SSRIs, for depression, anxiety and OCD), antipsychotics (for psychosis, severe autism irritability and some aggression), mood stabilisers (for bipolar disorder), and melatonin and alpha-2 agonists (for sleep and arousal). [13]
Your role as a general paediatrician is rarely to start complex psychotropic polypharmacy; it is to prescribe the common, evidence-based agents well, to monitor the developmental and metabolic consequences that show up in your clinic, and to coordinate with child and adolescent mental-health services (CAMHS) for the complex and the resistant. [1] [21]
Classification
Psychotropics used in youth sort cleanly by mechanism, and the mechanism explains both the benefit and the characteristic adverse-effect profile you must monitor. [13] [21]
Stimulants
Methylphenidate · amphetamines
- Block dopamine and noradrenaline reuptake in fronto-striatal circuits
- Same-day core-symptom effect on ADHD
- Schedule 8 / controlled drug — diversion and misuse risk
- Appetite suppression, sleep delay, growth, BP/HR, mood, tics
Non-stimulants
Atomoxetine · guanfacine XR · clonidine
- Noradrenaline reuptake inhibition (atomoxetine) or alpha-2 agonism
- Effect builds over weeks, not hours
- Not a controlled drug — preferred when diversion risk is high
- Sedation, BP/HR effects (alpha-2); GI upset, mood, rare hepatotoxicity (atomoxetine)
SSRIs
Fluoxetine · sertraline · escitalopram
- Serotonin reuptake inhibition; delayed antidepressant/anxiolytic effect
- Fluoxetine and sertraline dominate the paediatric evidence base
- Black-box suicidality warning in under-25s
- Activation, GI upset, hyponatraemia, discontinuation, serotonin syndrome
Antipsychotics (SGA)
Risperidone · aripiprazole
- D2 and 5-HT2A antagonism (aripiprazole partial agonist)
- Risperidone and aripiprazole for severe autism irritability; SGAs for early-onset psychosis
- Mandatory baseline and ongoing metabolic monitoring
- Weight gain, dyslipidaemia, hyperglycaemia, prolactin, EPS/sedation, QTc
Mood stabilisers
Lithium · valproate* · lamotrigine
- Lithium for bipolar prophylaxis; SGAs often first-line for acute mania
- Valproate highly teratogenic — avoid in girls of childbearing potential
- Lamotrigine for bipolar depression; slow titration to avoid rash
- Lithium: thyroid, renal, toxicity window; therapeutic drug monitoring
Melatonin / alpha-2
Melatonin · clonidine
- MT1/MT2 agonism advances circadian sleep onset (melatonin)
- Useful in ADHD/autism chronic sleep-onset insomnia after behavioural sleep
- Not controlled; relatively benign profile
- Behavioural sleep measures must always come first
A note on off-label use: much paediatric psychotropic prescribing is technically off-label because formal paediatric licensing trials lag behind clinical use. Off-label is not wrong, but it shifts the burden onto you to justify the indication, document the evidence, and monitor carefully. [21]
Epidemiology & Risk Factors
Prescribing of psychotropics to children and adolescents rose steeply in the 1990s and 2000s, plateaued or dipped after the 2004 FDA black-box warning on antidepressant suicidality, and has since risen again as depression, anxiety and ADHD presentations have grown. Stimulants are the most prescribed psychotropic in school-age children; SSRIs dominate adolescent prescribing; and antipsychotic use in youth — often off-label for aggression and irritability rather than for psychosis — has been a persistent safety concern because of its metabolic burden. [8] [21]
Headline numbers for viva
Children at highest risk of polypharmacy and adverse effects are those in out-of-home care, those with autism or intellectual disability, those with medical complexity, and adolescents with comorbid substance use. Sex, puberty and body composition also matter: hepatic enzyme maturation and changing fat stores shift the pharmacokinetics of lipophilic drugs across adolescence. [21]
Pathophysiology
Two layers matter: how the developing body handles the drug (pharmacokinetics), and how the drug's mechanism produces both benefit and adverse effect (pharmacodynamics). Get both right and you can predict onset, monitoring needs and drug-drug interactions without rote learning. [13] [17]
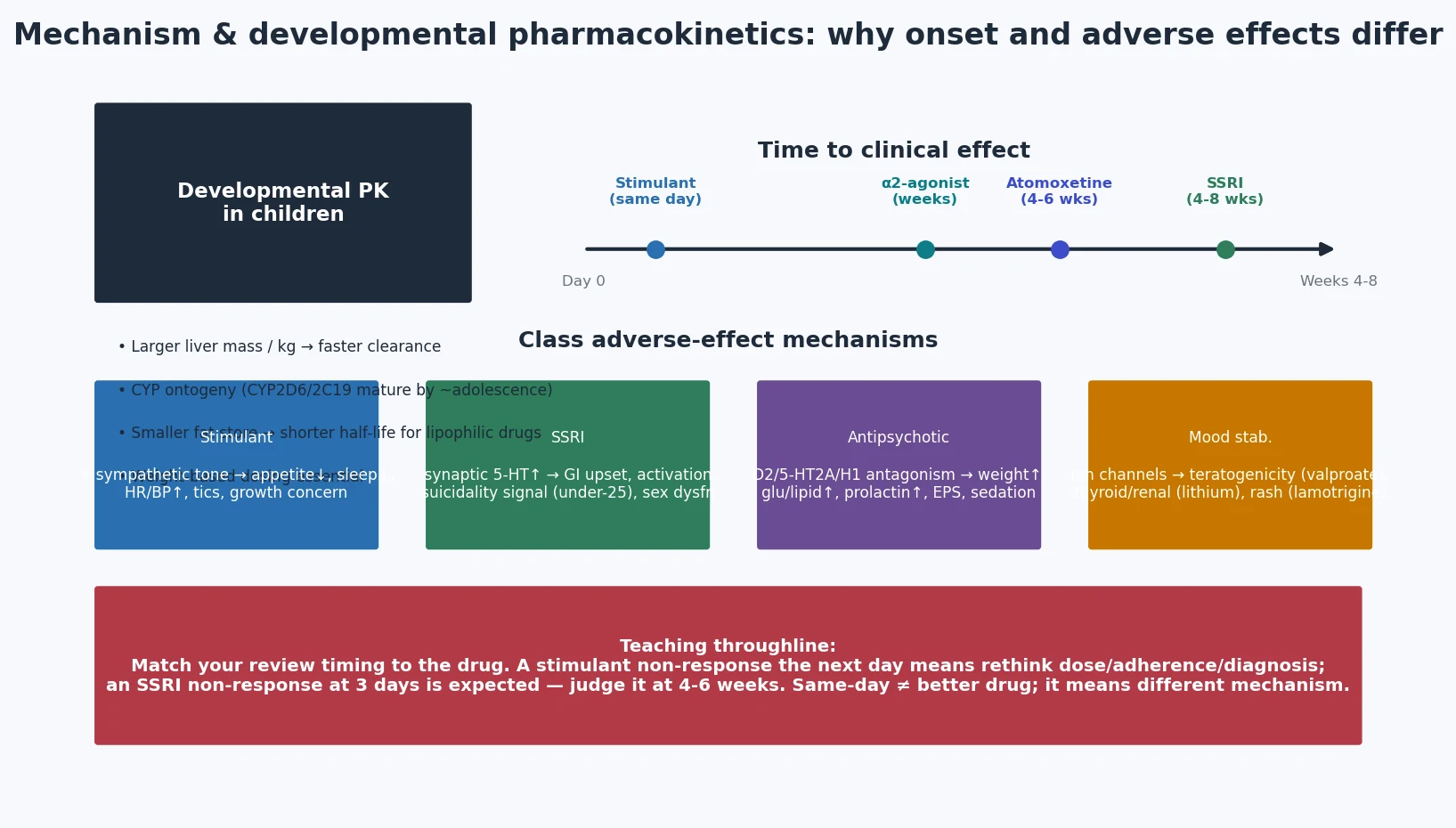
Developmental pharmacokinetics. Children have a larger liver mass per kilogram and a higher glomerular filtration rate, so they often clear drugs faster than adults on a per-kilogram basis; CYP enzyme ontogeny (particularly CYP2D6 and CYP2C19, which mature across childhood) changes exposure to atomoxetine, fluoxetine and many antipsychotics; and smaller fat stores shorten the half-life of lipophilic drugs. The practical consequence is that dosing must be weight-based and titrated, never simply copied from an adult dose. [14] [17]
Class mechanisms — the why behind the effect. Stimulants block dopamine and noradrenaline reuptake in fronto-striatal circuits, which is why core ADHD symptoms often improve within hours of an adequate dose. SSRIs block serotonin reuptake, but the antidepressant and anxiolytic effect emerges only over weeks as downstream receptor adaptation and neuroplasticity unfold — so an adolescent who feels no different at day 3 is on schedule, not failing treatment. Second-generation antipsychotics antagonise D2 and 5-HT2A receptors (aripiprazole is a partial agonist), helping psychosis and irritability but also driving weight gain through histamine H1 antagonism and prolactin elevation through D2 effects. Melatonin acts on MT1 and MT2 receptors in the suprachiasmatic nucleus to advance circadian phase, which is why it suits the delayed sleep phase common in ADHD and autism. [13] [23]
Drug-drug interactions arise from shared CYP pathways, additive QTc prolongation, and serotonergic or sedative additivity. Combining two QTc-prolonging psychotropics, adding a macrolide to an antipsychotic, or layering an SSRI onto tramadol can each precipitate serious harm; a quick interaction check is part of every polypharmacy review. [17]
Clinical Presentation
Children on psychotropics present to the general paediatrician in three ways: a scheduled review that is going well, a side-effect that has emerged, or a deterioration that you must not reflexively blame on the underlying illness. Each demands a different response. [12] [21]
| Presentation story | Do not stop here | Must still check |
|---|---|---|
| 'He's lost his appetite on the stimulant' | Appetite suppression is expected and common | Replot weight and height, review dose timing, consider a big breakfast, weight-band the dose, and weigh a formulation change |
| 'She feels worse on the fluoxetine' | Early worsening can be SSRI activation | Screen suicidality explicitly, ask for akathisia/activation, consider dose reduction or hold, safety-plan, and intensify review |
| 'He's gaining weight fast on risperidone' | Weight gain is a known antipsychotic effect | Replot BMI and waist, check fasting glucose and lipids, intensify lifestyle, and reconsider the agent if trajectory continues |
| 'She stopped the sertraline herself' | Non-adherence and abrupt cessation are common | Distinguish discontinuation syndrome from relapse; re-introduce or switch to fluoxetine and taper slowly |
| 'The tablets aren't working anymore' | Tolerance and non-response differ | Confirm adherence, dose, timing and diagnosis; check for new comorbidity, substance use or organic mimic |
The classic high-risk presentations are serotonin syndrome (agitation, tremor, hyperreflexia, clonus, autonomic instability and fever on a serotonergic agent) and neuroleptic malignant syndrome (fever, lead-pipe rigidity, autonomic instability and confusion on an antipsychotic). Both are emergencies: stop the drug, give supportive care, and escalate. [17] [22]
Differential Diagnosis
When a treated child deteriorates, the first question is not "what drug should I add?" but "is this the illness, the drug, or something else?" Run the deterioration through four buckets: disease progression, drug adverse effect, non-adherence, or a new mimic. [8] [21]
Disease progression
- Worsening depression despite an adequate 6–8 week SSRI trial
- Emerging bipolar depression or mixed state
- New comorbid anxiety, OCD or trauma
- Demands diagnosis re-evaluation, not automatic escalation
Drug adverse effect
- SSRI activation or akathisia within the first weeks
- Stimulant-induced irritability, anxiety or tic emergence
- Antipsychotic sedation mistaken for depression
- Serotonin syndrome or NMS — stop and escalate
Non-adherence
- Erratic effect, missed doses, parental conflict
- Adolescent stopping because of weight, sex or stigma effects
- Cost, access or formulation barriers
- Ask privately, without shame; rebuild the regimen
A new mimic
- Substance use, including cannabis and stimulants
- Thyroid dysfunction, iron deficiency, infection
- Bullying, safeguarding disclosure or family crisis
- Always re-take the history, not just the medication list
Two distinctions examiners probe: SSRI activation/akathisia versus worsening anxiety or emerging bipolar (activation tends to appear within the first weeks and includes inner restlessness and sleep disruption; a true bipolar switch needs manic symptoms, family history and specialist input); and stimulant-induced mood change versus comorbid anxiety, trauma or bipolar (rebound, dose-timing and afternoon mood matter). [8]
Clinical & Bedside Assessment
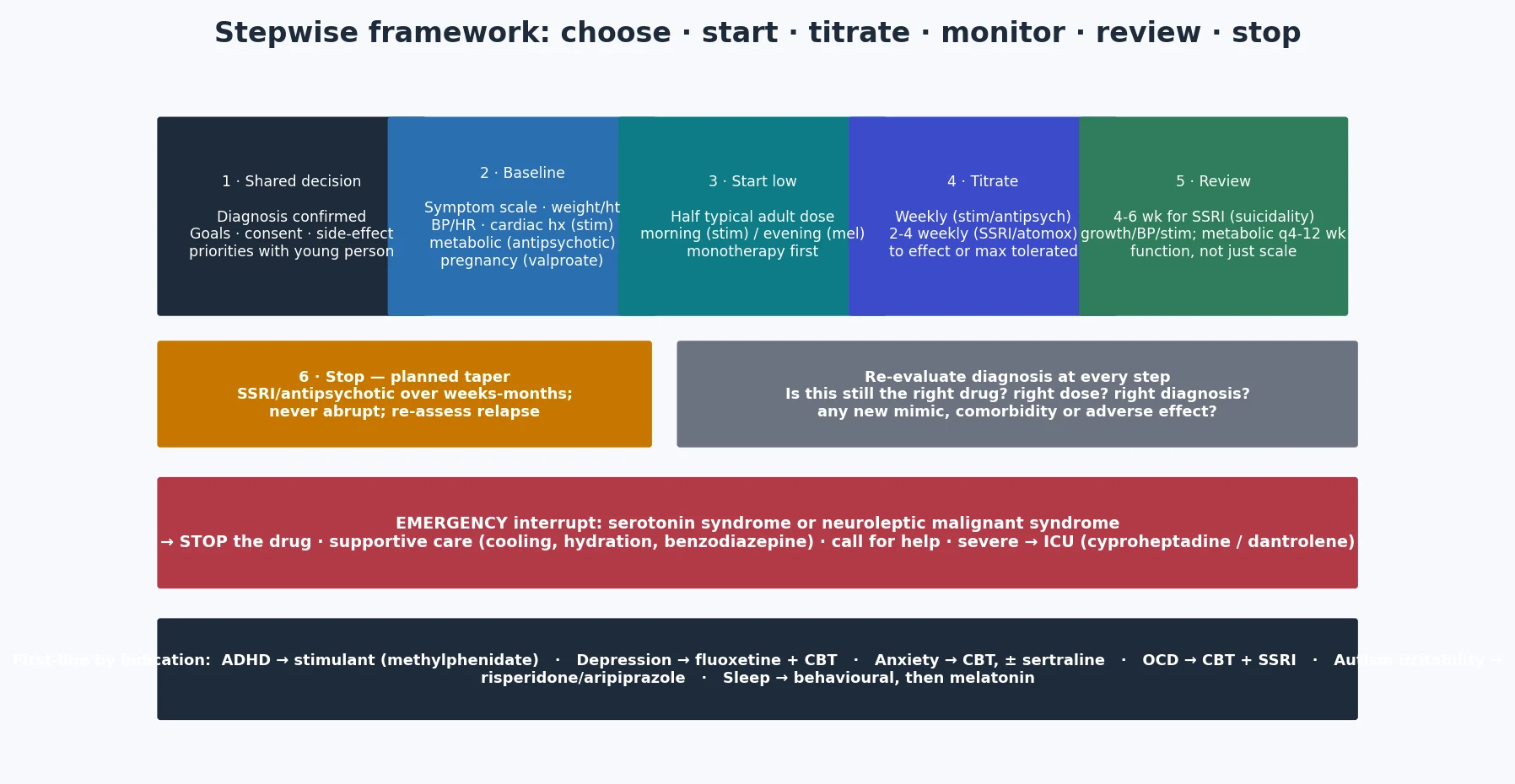
A structured pre-medication assessment prevents the most common and the most dangerous errors. Build the same sequence every time so nothing is omitted under time pressure. [12] [21]
Pre-medication and review assessment sequence
Confirm diagnosis and function
Multi-informant diagnosis, symptom-severity scale, functional impact, comorbidity screen — never start a psychotropic onto an unconfirmed label.
Baseline measures and safety screen
Weight, height, BMI, BP, HR; cardiac history before a stimulant; metabolic profile before an antipsychotic; pregnancy and contraception before valproate; bipolar/psychosis screen before an SSRI or stimulant.
Baseline rating scale
PHQ-A or similar for depression, GAD-7/SCARED for anxiety, Y-BOCS for OCD, Vanderbilt/Conners for ADHD, irritability and aberrant-behaviour scales for autism — to anchor later response.
Shared decision and consent
Goals, expected timeline, the suicidality warning for SSRIs, metabolic risk for antipsychotics, teratogenicity for valproate, side-effect priorities — with the young person, not just the parent.
Plan the review rhythm
Stimulant: weekly then monthly with growth, BP/HR, appetite, sleep, mood, tics. SSRI: 1 week, 2 weeks, 4 weeks and at every dose change for suicidality. Antipsychotic: metabolic monitoring at baseline, 4–6 weeks, 12 weeks, then quarterly.
Adherence, diversion and the adolescent voice
Private adolescent interview, pill or pharmacy reconciliation, diversion counselling, and a plan the young person actually endorses.
Use professional interpreters for language-discordant families; consent quality and adherence both fall when a child translates. For Indigenous, migrant and out-of-home-care families, culturally safe communication and an explicit trauma history change both the choice and the monitoring. [21]
Investigations
There is no single blood panel for "starting a psychotropic." Investigations are targeted by class and by the specific safety question. [16] [21]
Before a stimulant. Plot height and weight, measure blood pressure and heart rate with an appropriate cuff, and take a personal cardiac history (exertional chest pain, unexplained syncope, palpitations) and a family history of sudden cardiac death or serious arrhythmia. Large cohort data have not shown a population excess of serious cardiovascular events with ADHD drugs, but individual risk assessment still matters; an ECG is used when history or examination raises concern rather than as a universal reflex. [16] [17]
Before an antipsychotic. Baseline weight, height, BMI and waist circumference, blood pressure, fasting glucose or HbA1c, and a fasting lipid profile — repeated at 4–6 weeks, 12 weeks, and then at least quarterly for weight/BMI and annually for glucose and lipids. Consider a baseline prolactin and ECG when the agent or combination is QTc-relevant. [21] [22]
Before valproate in a girl of childbearing potential. Pregnancy test, contraception counselling, and engagement with the pregnancy-prevention programme (PPP); document the teratogenicity and neurodevelopmental risk discussion explicitly. Lithium requires baseline renal and thyroid function and a therapeutic level. [21]
Symptom-rating scales (PHQ-A, GAD-7, SCARED, Y-BOCS, Vanderbilt, Conners) track response and belong at every review, not just at the start. [1] [12]
Management — Resuscitation
Psychotropic emergencies are uncommon but dangerous, and the general paediatrician must recognise them and act before the specialist arrives. The emergencies are serotonin syndrome, neuroleptic malignant syndrome, acute SSRI-induced suicidality or activation, severe extrapyramidal reaction or acute dystonia, and QTc-related collapse. [17] [22]
The single most common resuscitation trap is dismissing new agitation or suicidal thoughts as "just the underlying illness" in an adolescent recently started on an SSRI. The FDA black-box warning exists for a reason: ask about suicidal thoughts explicitly at every early review. [8] [9]
Management — Definitive & Stepwise
Definitive management is the art of choosing the right first-line agent, starting low and titrating slowly, monitoring the consequences, and stopping thoughtfully. The framework is the same across classes; only the agent, the onset and the monitoring change. [1] [12] [21]
ADHD medicines
The Cortese network meta-analysis found that stimulants (particularly methylphenidate) had the largest effect on core ADHD symptoms in children and adolescents at around 12 weeks, while the Storebø Cochrane review confirms methylphenidate efficacy while flagging study-quality limits. Methylphenidate is commonly first-line; amphetamine-class agents (including lisdexamfetamine) are alternatives. [13] [12]
| Agent class | Typical start framework | Titration / range notes | Key teaching points |
|---|---|---|---|
| Methylphenidate | Immediate-release ~0.3 mg/kg (or product-specific 5 mg) in the morning | Titrate weekly to effect and tolerance; modified-release products for school-day coverage | Same-day effect; appetite, sleep, growth, BP/HR, mood, tics; confirm dose locally [12] |
| Amphetamines | Low product-specific morning start | Titrate weekly; lisdexamfetamine once daily | Alternative or second-line; similar monitoring; diversion risk [13] |
| Atomoxetine | ~0.5 mg/kg/day orally for at least 3 days | Increase toward ~1.2 mg/kg/day; usual max ~1.4 mg/kg/day or 100 mg/day | Effect over weeks; useful when diversion risk high; monitor mood, GI, rare hepatotoxicity [14] |
| Guanfacine XR | 1 mg orally once daily | Increase by 1 mg weekly; trial ranges 1–4 mg/day (higher adolescent maxima) | Useful when tics, sleep-onset problems or aggression; monitor sedation, BP, HR; taper after prolonged use [15] |
Onset teaching point. Stimulant benefit on core symptoms is often evident the same day at an adequate dose, while atomoxetine builds over 4–6 weeks — judge early non-response accordingly. [13] [14]
SSRIs for depression, anxiety and OCD
Fluoxetine has the strongest paediatric evidence base and is the SSRI approved by the FDA for depression down to age 8; sertraline has strong evidence for childhood anxiety (CAMS) and OCD. The pivotal TADS trial showed that fluoxetine, cognitive-behavioural therapy and their combination all beat placebo for adolescent depression, with combination therapy lowering suicidality compared with fluoxetine alone — the central teaching that medication plus therapy is safer and better than medication alone. [1] [2] [5] [6]
| Indication | First-line framework | Evidence anchor | Key monitoring |
|---|---|---|---|
| Adolescent major depression | Fluoxetine first-line, ideally with CBT | TADS (fluoxetine + CBT) [1] | Suicidality at 1, 2, 4 weeks and at dose change; response at 4–6 weeks |
| Childhood anxiety | CBT first; sertraline or fluoxetine adjunct | CAMS (sertraline ± CBT) [5] | Activation, GI upset, response at 4–6 weeks |
| Paediatric OCD | CBT plus an SSRI (sertraline/fluoxetine/fluvoxamine) | POTS (sertraline + CBT) [6] | Dose to response; relapse on early cessation; longer trials |
| SSRI-resistant depression | Optimise dose and adherence; switch or augment with CBT | TORDIA [7] | Re-screen diagnosis and comorbidity; specialist CAMHS |
The suicidality warning. The FDA black-box warning applies to all antidepressants in people aged under 25. The Bridge meta-analysis found an increased risk of reported suicidal ideation and attempts in paediatric antidepressant trials, while the Gibbons reanalysis suggested the absolute risk is low and that effective treatment of depression itself protects against suicide. The defensible exam position is: monitor suicidality closely in the first four weeks and at every dose change, but do not let the warning cause undertreatment of real depression, because untreated depression carries its own substantial suicide risk. [8] [9]
What not to use first-line. Paroxetine, venlafaxine and tricyclic antidepressants should not be first-line for paediatric depression: the original Study 329 claimed efficacy for paroxetine in adolescents but the Restoring Study 329 reanalysis found the benefit was overstated and the harms understated, a landmark example of publication bias in paediatric psychopharmacology. [10]
Antipsychotics for autism irritability and early-onset psychosis
For severe irritability and aggression in autism that has not responded to behavioural and educational intervention, risperidone and aripiprazole have randomised controlled evidence. The RUPP trial established risperidone for serious behavioural problems in children with autism, and the Marcus and Owen fixed-dose trials established aripiprazole for autistic irritability. The trade is metabolic: weight gain, dyslipidaemia and hyperglycaemia are common, so behavioural failure is the threshold, not parental preference for a tablet. [18] [19] [20]
The Correll first-use study quantified the cardiometabolic risk of second-generation antipsychotics in children: weight gain and metabolic change were substantial over the first 11 weeks, with olanzapine highest and aripiprazole among the lower, and even agents considered "metabolically safer" produced clinically significant change. The Ray cohort study linked antipsychotic treatment in children and youths to a higher risk of unexpected death — a finding that sharpens the need for clear indication, monitoring and time-limiting. [21] [22]
WEIGHT
Mood stabilisers and valproate
For acute bipolar mania in an adolescent, a second-generation antipsychotic is often first-line, with lithium for prophylaxis and lamotrigine for bipolar depression. Valproate must not be used in a girl of childbearing potential without a pregnancy-prevention programme: it is highly teratogenic (neural tube defects) and associated with neurodevelopmental disorders in exposed children. Lithium requires renal and thyroid monitoring and has a narrow therapeutic window, so drug-level monitoring guides dose. [21] [22]
Melatonin and sleep
For chronic sleep-onset insomnia in ADHD or autism that has not responded to behavioural sleep measures, melatonin advances sleep onset and total sleep time. Van der Heijden showed melatonin improved sleep in children with ADHD and chronic sleep-onset insomnia, and Malow reported that two years of prolonged-release melatonin in children with autism sustained sleep benefit without disrupting growth or puberty. Behavioural sleep measures — consistent bedtime, screen-off, sleep hygiene — must always come first. [23] [24]
Melatonin (paediatric sleep-onset insomnia, after behavioural sleep)
Dose
~0.5–6 mg orally, 30–60 minutes before bedtime
Australian and New Zealand practice follows state stimulant prescribing authorities (which vary by jurisdiction and age) and shared-care norms: specialist initiation or endorsement where required, documented diagnosis, monitoring plan, and GP shared care when stable. The RANZCP provides professional practice guidance on psychotropic prescribing. Always confirm doses against the AMH Children's Dose Companion and local product information. [12]
Specific Subtypes & Scenarios
School-age moderate-to-severe ADHD. A long-acting methylphenidate product with weekly titration, classroom supports and parent behavioural training is the standard first approach, with atomoxetine or guanfacine XR as alternatives. [12] [13]
Adolescent major depression. Fluoxetine with CBT is first-line for moderate-to-severe depression; review at 1, 2 and 4 weeks for suicidality and at 6 weeks for response; switch or augment per TORDIA if resistant. [1] [7]
Childhood anxiety disorder. CBT first; add sertraline or fluoxetine when anxiety is moderate-to-severe or impairing — combination was best in CAMS. [5]
Paediatric OCD. CBT plus an SSRI (sertraline, fluoxetine or fluvoxamine); dose to response and treat for an adequate duration before declaring non-response. [6]
Severe autism irritability. After behavioural and educational intervention has failed, risperidone or aripiprazole with mandatory metabolic monitoring; set a clear target and a plan to trial off. [18] [19] [20]
Early-onset psychosis. Specialist CAMHS; a second-generation antipsychotic with metabolic and prolactin monitoring and a recovery-oriented plan. [21]
Adolescent bipolar disorder. Second-generation antipsychotic for acute mania, lithium for prophylaxis, lamotrigine for bipolar depression; avoid valproate in girls of childbearing potential without a PPP. [21]
Adolescent girl of childbearing potential. Treat valproate as a last resort; contraception and a pregnancy-prevention programme are mandatory where it cannot be avoided. [21]
Sleep-onset insomnia in ADHD or autism. Behavioural sleep first, then melatonin; sustained benefit has been shown without disrupting growth or puberty. [23] [24]
Preschool child. Psychoeducation and behavioural intervention first; medication only specialist-led after behavioural therapy has failed or is unavailable. [12]
Child in out-of-home care with polypharmacy. High risk of overprescription and drug-drug interaction; indication review, deprescribing and a trauma-informed plan are the priorities, often led jointly with CAMHS. [21]
Complications & Pitfalls
Classic errors include starting an SSRI without informing the family about the suicidality warning; prescribing an antipsychotic without baseline or ongoing metabolic monitoring; using paroxetine, venlafaxine or tricyclics first-line for paediatric depression despite weaker evidence and harm signals; prescribing valproate to an adolescent girl without contraception; misjudging early non-response by treating a same-day stimulant and a weeks-long SSRI the same way; stopping SSRIs or antipsychotics abruptly; missing SSRI activation mislabelled as worsening anxiety; failing to monitor growth, blood pressure and appetite on stimulants; and combining QTc-prolonging psychotropics without ECG awareness. [8] [10] [21]
The deeper pitfall is relying on medication alone. Every drug class in this topic works better alongside psychoeducation, psychological therapy, school and family support; the multimodal evidence (TADS combination; CAMS combination) consistently favours combined care over medication in isolation. [1] [5]
Prognosis & Disposition
A good response is defined by function — school attendance, peer and family relationships, mood, sleep, safety — not only a symptom-scale score. The duration of treatment depends on the condition: ADHD stimulant treatment may continue for years with monitoring; a first episode of adolescent depression is typically treated for 6–12 months after remission before a monitored trial off; OCD often requires longer SSRI duration; and autism irritability treated with an antipsychotic should be reviewed regularly with a plan to trial off the lowest effective dose. [1] [6] [21]
The long-term cardiometabolic outlook for a child on an antipsychotic is materially shaped by monitoring and lifestyle intervention; early weight-gain trajectory predicts later metabolic risk, so the first three months matter. Disposition ranges from shared primary care for stable stimulant or SSRI treatment to specialist CAMHS for resistant depression, early-onset psychosis, bipolar disorder and complex polypharmacy. Transition to adult services must transfer prescribing ownership, monitoring responsibility and adherence support deliberately, not by default. [21] [22]
Special Populations
Preschool children deserve behavioural intervention first; psychotropic medication is exceptional and specialist-led. Adolescents bring autonomy, confidentiality, consent, adherence, diversion, pregnancy and substance-use considerations into every prescription. Girls of childbearing potential carry the valproate constraint and need contraception and PPP counselling. Children with autism and intellectual disability need communication access, behavioural-first care, lower antipsychotic doses and the same metabolic monitoring as any other child. Children in out-of-home care are at highest risk of polypharmacy and need trauma-informed, indication-led prescribing and deprescribing. Indigenous and migrant families need culturally safe prescribing and interpreter-supported consent. Rural and remote care can use telehealth for follow-up but still needs reliable measurement of weight, blood pressure and adherence with clear shared-care ownership. [21] [23]
Evidence, Guidelines & Regional Differences
TADS one-liner. Fluoxetine, CBT and their combination all beat placebo for adolescent depression; combination therapy gave the best outcomes and lowered suicidality compared with fluoxetine alone — the cornerstone evidence that medication plus therapy is safer and better than medication alone. [1] [2]
Suicidality-signal one-liner. Bridge's meta-analysis found an increased risk of reported suicidal ideation and attempts in paediatric antidepressant trials; Gibbons's reanalysis argued the absolute risk is low and that effective treatment itself protects. The defensible position is close monitoring plus treatment, not avoidance. [8] [9]
Antipsychotic metabolic one-liner. Correll showed substantial weight gain and metabolic change in the first 11 weeks of first-time paediatric antipsychotic use, with olanzapine highest and aripiprazole among the lower; Ray linked antipsychotic treatment to higher unexpected-death risk in children and youths — both demand clear indication, monitoring and a plan to trial off. [21] [22]
Publication-bias one-liner. Restoring Study 329 showed the original paroxetine-in-adolescents trial overstated benefit and understated harm — the reason paroxetine is not first-line for paediatric depression and why you read the reanalysis, not just the headline. [10]
Where evidence is strong: stimulants for ADHD, fluoxetine and sertraline for the common youth internalising disorders, risperidone and aripiprazole for severe autism irritability. Where it is weaker: antipsychotics for generic aggression, psychotropic polypharmacy, and many off-label uses in preschool children. [13] [21]
Exam Pearls
PRESCRI
Self-test: adolescent starting fluoxetine for moderate depression
Confirm diagnosis and severity (PHQ-A), screen for bipolar/psychosis and suicidal ideation, take baseline weight and examine; start fluoxetine at half the typical adult dose, ideally with CBT; review at 1 week, 2 weeks and 4 weeks for suicidality and activation, and at 6 weeks for response; counsel explicitly about the black-box warning, the expected 4–6 week onset, and common side effects (GI upset, sleep change, activation); give the family a safety plan and an open-access pathway; and arrange shared care with CAMHS. [1] [2] [8]
References
- [1]March J Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents with Depression Study (TADS) randomized controlled trial. JAMA, 2004.PMID 15315995
- [2]March JS The Treatment for Adolescents With Depression Study (TADS): long-term effectiveness and safety outcomes. Archives of General Psychiatry, 2007.PMID 17909125
- [3]Emslie G Treatment for Adolescents with Depression Study (TADS): safety results. Journal of the American Academy of Child and Adolescent Psychiatry, 2006.PMID 17135989
- [4]Emslie GJ A double-blind, randomized, placebo-controlled trial of fluoxetine in children and adolescents with depression. Archives of General Psychiatry, 1997.PMID 9366660
- [5]Walkup JT Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine, 2008.PMID 18974308
- [6]Pediatric OCD Treatment Study (POTS) Team Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA, 2004.PMID 15507582
- [7]Brent D Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial. JAMA, 2008.PMID 18314433
- [8]Bridge JA Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA, 2007.PMID 17440145
- [9]Gibbons RD Suicidal thoughts and behavior with antidepressant treatment: reanalysis of the randomized placebo-controlled studies of fluoxetine and venlafaxine. Archives of General Psychiatry, 2012.PMID 22309973
- [10]Le Noury J Restoring Study 329: efficacy and harms of paroxetine and imipramine in treatment of major depression in adolescence. BMJ, 2015.PMID 26376805
- [11]Cipriani A Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet, 2018.PMID 29477251
- [12]Storebø OJ Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD). Cochrane Database of Systematic Reviews, 2023.PMID 36971690
- [13]Cortese S Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry, 2018.PMID 30097390
- [14]Michelson D Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study. American Journal of Psychiatry, 2002.PMID 12411225
- [15]Sallee FR Guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder: a placebo-controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 2009.PMID 19106767
- [16]Cooper WO ADHD drugs and serious cardiovascular events in children and young adults. New England Journal of Medicine, 2011.PMID 22043968
- [17]Hennissen L Cardiovascular Effects of Stimulant and Non-Stimulant Medication for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Trials of Methylphenidate, Amphetamines and Atomoxetine. CNS Drugs, 2017.PMID 28236285
- [18]McCracken JT Risperidone in children with autism and serious behavioral problems. New England Journal of Medicine, 2002.PMID 12151468
- [19]Marcus RN A placebo-controlled, fixed-dose study of aripiprazole in children and adolescents with irritability associated with autistic disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2009.PMID 19797985
- [20]Owen R Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics, 2009.PMID 19948625
- [21]Correll CU Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents. JAMA, 2009.PMID 19861668
- [22]Ray WA Association of Antipsychotic Treatment With Risk of Unexpected Death Among Children and Youths. JAMA Psychiatry, 2019.PMID 30540347
- [23]Van der Heijden KB Effect of melatonin on sleep, behavior, and cognition in ADHD and chronic sleep-onset insomnia. Journal of the American Academy of Child and Adolescent Psychiatry, 2007.PMID 17242627
- [24]Malow BA Sleep, Growth, and Puberty After 2 Years of Prolonged-Release Melatonin in Children With Autism Spectrum Disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2021.PMID 31982581