Ankylosing Spondylitis
AS is strongly associated with HLA-B27 positivity (present in 85-95% of patients), though only 1-5% of HLA-B27-positive individuals develop the disease, indicating additional genetic and environmental factors are...
What matters first
AS is strongly associated with HLA-B27 positivity (present in 85-95% of patients), though only 1-5% of HLA-B27-positive individuals develop the disease, indicating additional genetic and environmental factors are...
Chalk Stick Fracture -> Unstable fracture after minor trauma
6 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Chalk Stick Fracture -> Unstable fracture after minor trauma
- Cauda Equina Syndrome -> Late complication of dural ectasia
- Anterior Uveitis -> Urgent Ophthalmology
- Aortic Regurgitation -> Chest Pain / Dyspnoea
Linked comparisons
Differentials and adjacent topics worth opening next.
- Mechanical Back Pain
- Psoriatic Arthritis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Ankylosing Spondylitis
1. Clinical Overview
Summary
Ankylosing Spondylitis (AS) is a chronic seronegative inflammatory spondyloarthropathy characterized by inflammation of the axial skeleton (sacroiliitis and spondylitis) and entheses. It is the prototype of the axial spondyloarthritis (axSpA) spectrum, which includes radiographic AS (r-axSpA) and non-radiographic axSpA (nr-axSpA). The disease typically affects young adults in their second to third decade, with a male predominance of approximately 2-3:1. [1,2]
AS is strongly associated with HLA-B27 positivity (present in 85-95% of patients), though only 1-5% of HLA-B27-positive individuals develop the disease, indicating additional genetic and environmental factors are required. [3] The hallmark clinical feature is inflammatory back pain characterized by insidious onset, morning stiffness exceeding 30 minutes, improvement with exercise but not rest, pain at night (second half), and alternating buttock pain. [4]
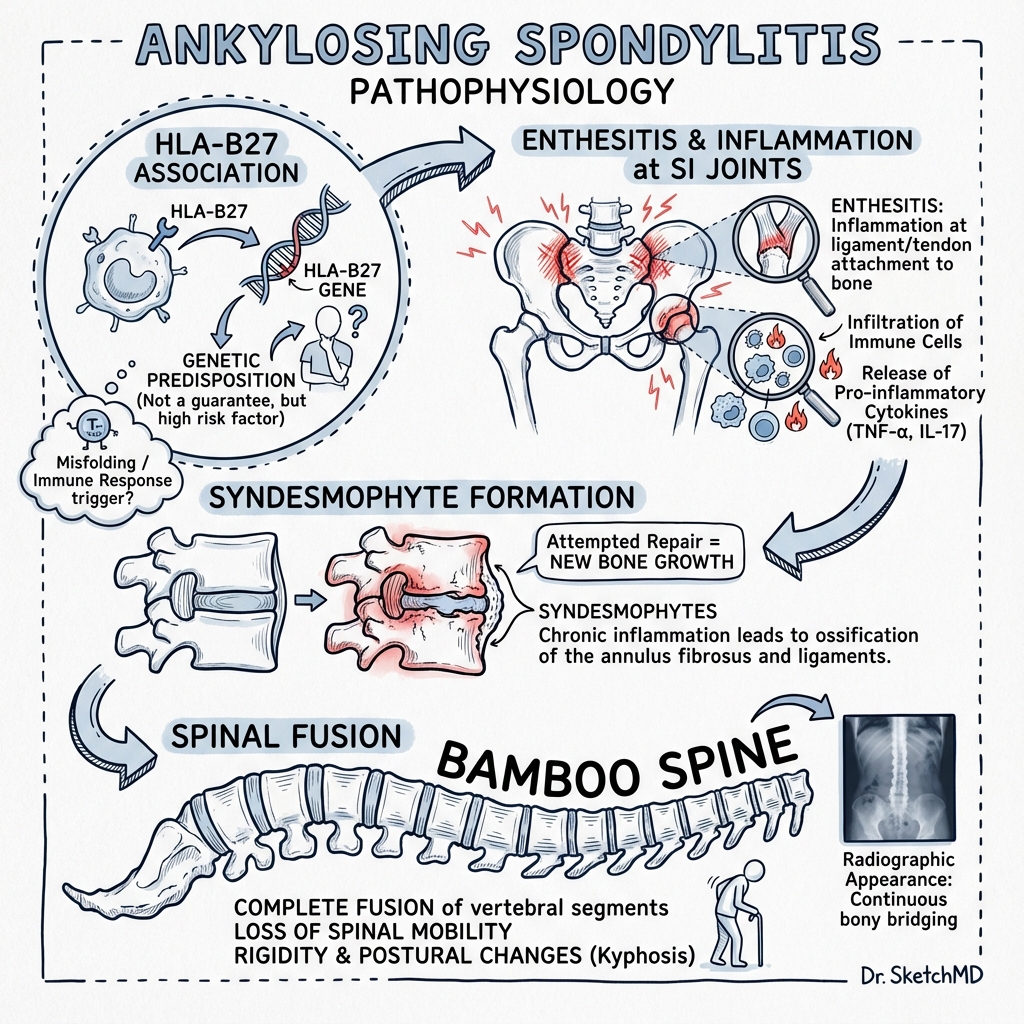
The natural history involves progressive ossification and fusion of the spine, creating the characteristic "bamboo spine" appearance on radiographs. This process results from chronic inflammation at entheses (enthesitis), followed by erosion, reactive bone formation (syndesmophytes), and eventual ankylosis. The fused spine becomes rigid and osteoporotic, predisposing to catastrophic "chalk stick fractures" following minor trauma. [5,6]
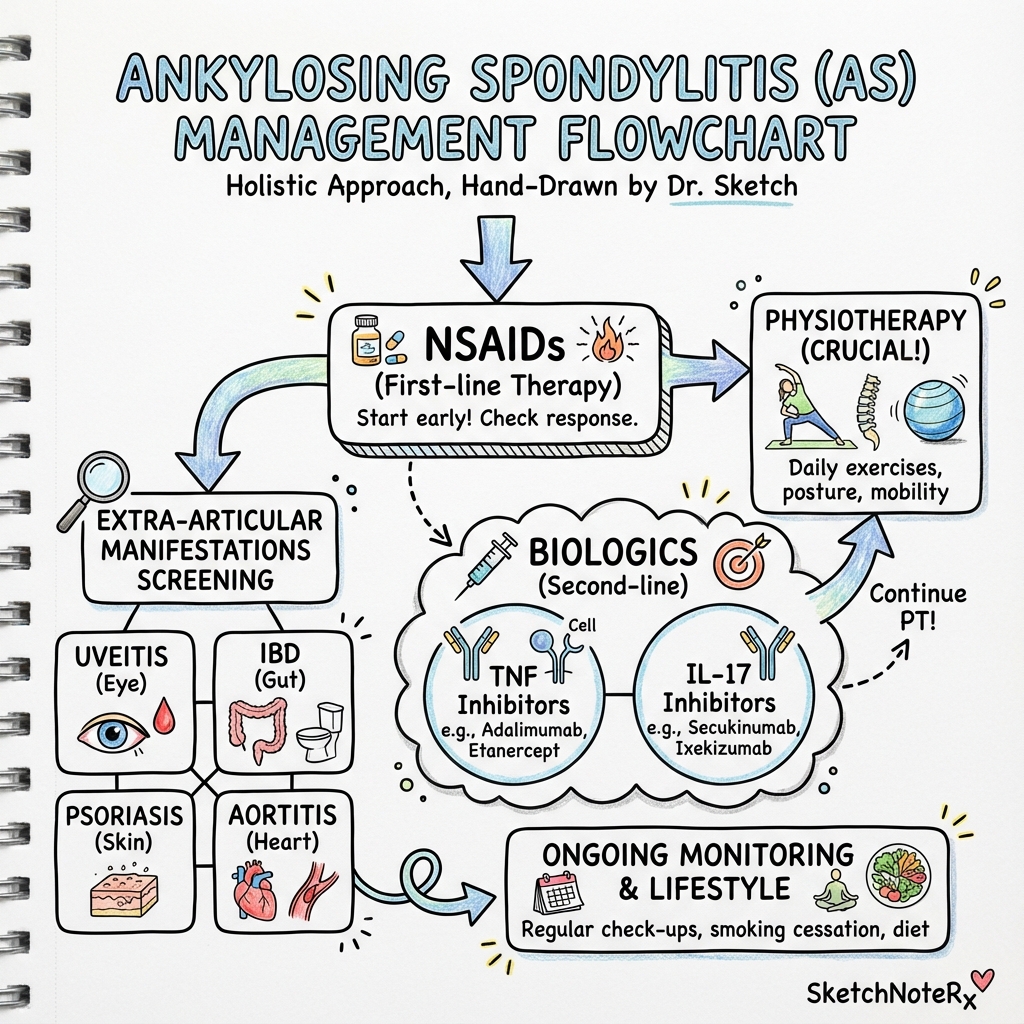
Management has been revolutionized by biological therapies, particularly TNF inhibitors and IL-17 inhibitors, which can dramatically reduce disease activity and potentially slow radiographic progression when initiated early. However, non-pharmacological interventions including physiotherapy and exercise remain cornerstones of treatment throughout the disease course. [7,8]
Key Facts
- The "Question Mark" Posture: Progressive loss of lumbar lordosis combined with increased thoracic kyphosis and compensatory cervical hyperextension creates a characteristic stooped-forward appearance resembling a question mark in profile.
- The 3 A's: Classic extra-articular manifestations: Anterior Uveitis (25-30%), Aortic Regurgitation (2-10%), Apical Lung Fibrosis (1-2%).
- Inflammatory vs Mechanical Back Pain:
- Inflammatory: Age less than 40 years, Insidious onset, Morning stiffness > 30min, Improvement with exercise, No improvement with rest, Pain at night (second half).
- Mechanical: Age > 40 years, Acute/traumatic onset, Stiffness less than 30min, Worse with activity, Better with rest, No night pain.
- Seronegative Spondyloarthropathy: Rheumatoid factor (RF) and anti-CCP antibodies are negative, distinguishing AS from rheumatoid arthritis.
- Bath Indices: Disease activity measured by BASDAI (Bath Ankylosing Spondylitis Disease Activity Index); function by BASFI (Bath Ankylosing Spondylitis Functional Index); metrology by BASMI (Bath Ankylosing Spondylitis Metrology Index).
Clinical Pearls
"The Chalk Stick Fracture": An AS patient who falls from standing height and complains of neck or back pain has a fracture until proven otherwise. The ankylosed spine is rigid and osteoporotic, snapping transversely like chalk. These are highly unstable three-column fractures with significant risk of spinal cord injury. CT of the entire spine is mandatory—plain radiographs miss up to 30% of fractures due to distorted anatomy and overlying ossification. [9]
"Don't Intubate Blindly": The cervical spine in advanced AS is often fused in flexion with reduced atlanto-occipital extension. Attempting conventional laryngoscopy with neck extension can cause catastrophic spinal cord injury. Awake fibreoptic intubation with the patient in their habitual position is the safe approach. Pre-operative anaesthetic assessment and documentation of neck mobility is critical. [10]
"Wall Test": Ask the patient to stand with heels and back against a wall while maintaining a forward gaze. Measure the occiput-to-wall distance. In normal individuals, the occiput touches the wall (0cm). In AS with thoracic kyphosis and loss of lumbar lordosis, the occiput cannot reach the wall. Distance > 0cm indicates spinal deformity and correlates with disease severity.
"Morning Stiffness is the Barometer": The duration and severity of morning stiffness directly reflects disease activity. Patients often describe needing to "get the engine started" with a hot shower and gentle movement. Effective treatment dramatically reduces this symptom within weeks.
"Plantar Fasciitis in a Young Man = Think SpA": Enthesitis (inflammation at tendon/ligament insertions) is a hallmark feature. Plantar fasciitis, Achilles tendinitis, or costochondritis in a young adult should trigger consideration of spondyloarthritis, especially with associated back symptoms.
2. Epidemiology
Prevalence and Incidence
The prevalence of AS varies significantly by geographic region and ethnic group, largely paralleling the prevalence of HLA-B27 in the population. [11]
- Global Prevalence: 0.1-1.4% of the general population, with highest rates in northern European populations and Native American groups.
- UK Prevalence: Approximately 0.5%, affecting ~400,000 individuals.
- Incidence: 0.4-14 per 100,000 person-years.
- HLA-B27 Prevalence:
- Caucasians: 6-8%
- East Asian: 4-6%
- Sub-Saharan African: less than 1%
- Native American (Haida): Up to 50%
Demographics
- Age of Onset: Peak onset 20-30 years. Symptom onset > 45 years is uncommon and should prompt consideration of alternative diagnoses.
- Gender Ratio: Historically reported as 3:1 male predominance. Recent studies suggest closer to 2:1, with women often having milder disease, delayed diagnosis, and more peripheral arthritis.
- Genetic Risk:
- HLA-B27 positive: Relative risk 50-100 compared to HLA-B27 negative individuals.
- First-degree relative with AS: 10-30% lifetime risk if HLA-B27 positive; less than 5% if HLA-B27 negative.
- Monozygotic twins: 63% concordance.
- HLA-B27 accounts for ~30% of genetic susceptibility; non-HLA genes (ERAP1, IL23R) contribute additional risk. [12]
Natural History
- Diagnostic Delay: Average 5-10 years from symptom onset to diagnosis, often longer in women.
- Radiographic Progression: Sacroiliitis typically precedes spinal involvement. Syndesmophytes develop in 30-50% of patients within 10 years.
- Functional Limitation: 30-40% of patients develop significant functional impairment over 20-30 years.
- Work Disability: Up to 50% of patients experience work disability by 15 years from diagnosis in pre-biologic era studies. [13]
3. Pathophysiology
Genetic Factors
HLA-B27
HLA-B27 is present in 85-95% of AS patients compared to 6-8% of the general Caucasian population. However, only 1-5% of HLA-B27-positive individuals develop AS, indicating additional factors are required. [3]
Proposed Mechanisms:
- Arthritogenic Peptide Theory: HLA-B27 presents specific bacterial peptides to CD8+ T cells, triggering autoimmune response against self-antigens with molecular mimicry.
- Misfolding Theory: HLA-B27 heavy chains misfold in the endoplasmic reticulum, triggering unfolded protein response (UPR), leading to IL-23 production and Th17 activation.
- Homodimer Formation: HLA-B27 heavy chain homodimers (without β2-microglobulin) are recognized by killer immunoglobulin-like receptors (KIR), activating innate immune cells. [14]
Non-HLA Genes
Genome-wide association studies (GWAS) have identified > 100 genetic loci associated with AS:
- ERAP1 (Endoplasmic Reticulum Aminopeptidase 1): Trims peptides for HLA presentation; polymorphisms interact with HLA-B27.
- IL23R: Receptor for IL-23, critical for Th17 differentiation.
- IL12B, IL6R, TNFR1, CARD9: Genes involved in innate immunity and inflammatory pathways. [12]
Immunopathogenesis
The inflammatory cascade in AS involves:
- Initiating Event: Unknown trigger (possibly gut microbiome dysbiosis) in genetically susceptible individual.
- IL-23/IL-17 Axis: IL-23 promotes differentiation of Th17 cells, which produce IL-17A, IL-17F, and IL-22. These cytokines drive inflammation at entheses.
- TNF-α: Central pro-inflammatory cytokine; drives both inflammation and new bone formation.
- Enthesitis: Primary pathological lesion occurs at entheses (bone-tendon/ligament junctions), particularly at vertebral corners where annulus fibrosus attaches.
- Osteoproliferation: Inflammatory cytokines paradoxically stimulate bone formation via BMP (bone morphogenetic protein) and Wnt signaling pathways, creating syndesmophytes. [15]
Pathological Sequence
Early Disease (Inflammatory Phase):
- Enthesitis: Inflammation at annulus fibrosus insertion → vertebral corner.
- Spondylitis: Extension into vertebral body → bone marrow edema (visible on MRI STIR sequences).
- Spondylodiscitis: Erosion at discovertebral junction → Romanus lesions ("shiny corners").
- Sacroiliitis: Bilateral inflammation of sacroiliac joints → erosions, sclerosis.
Late Disease (Proliferative Phase):
- Syndesmophyte Formation: Vertical ossification bridging vertebral bodies (distinguishes from DISH, which has flowing anterior ossification).
- Ankylosis: Complete fusion of:
- Sacroiliac joints
- Apophyseal (facet) joints
- Costovertebral joints → restricted chest expansion
- Discovertebral junctions
- "Bamboo Spine": Continuous vertical fusion creating rigid structure.
- Osteoporosis: Immobilization and chronic inflammation → decreased bone mineral density → fracture risk. [16]
The "Mechanical Stress" Hypothesis
AS preferentially affects high-stress mechanical sites: sacroiliac joints (transmit upper body weight), lumbar spine (maximal motion), and entheses subject to repetitive stress. This suggests mechanical factors may amplify inflammatory responses at these locations.
4. Clinical Presentation
Symptoms
Inflammatory Back Pain (IBP)
The defining clinical feature, present in > 90% of patients. Berlin Criteria for IBP (≥2 of 4):
- Age of onset less than 40 years
- Insidious onset
- Improvement with exercise
- No improvement with rest
- Night pain (particularly second half of night, improves on getting up)
Additional features:
- Morning Stiffness: Duration > 30 minutes, often 1-2 hours. Described as "gelling"—stiffness after inactivity.
- Alternating Buttock Pain: Suggests sacroiliitis; pain radiates from sacrum to posterior thigh, mimicking sciatica but lacking radicular features.
- Duration: Symptoms must be present for ≥3 months to meet diagnostic criteria. [4]
Peripheral Manifestations
- Peripheral Arthritis: 25-30% develop peripheral joint involvement, typically asymmetric, oligoarticular, affecting lower limbs (hips, knees, ankles).
- Enthesitis: 30-50% experience entheseal inflammation:
- Achilles tendinitis
- Plantar fasciitis
- Costochondritis (chest wall pain)
- Greater trochanteric bursitis
- Ischial tuberosity tenderness
- Dactylitis: "Sausage digit"—diffuse swelling of entire finger/toe; seen in 5-10%, more common in psoriatic arthritis.
Extra-Articular Manifestations
Anterior Uveitis (25-30%)
- Most common extra-articular feature; lifetime prevalence 25-30%.
- Presentation: Acute onset unilateral painful red eye, photophobia, blurred vision.
- Typically anterior, non-granulomatous, recurrent, alternating eyes.
- Requires urgent ophthalmology assessment → topical corticosteroids.
- Strongly associated with HLA-B27 (50% of acute anterior uveitis is HLA-B27 related). [17]
Cardiovascular (2-10%)
- Aortitis: Inflammation of aortic root → dilation → aortic regurgitation.
- Conduction Defects: AV blocks, bundle branch blocks.
- Increased CV Risk: Chronic inflammation increases atherosclerosis risk (2-fold).
Pulmonary (1-2%)
- Apical Lung Fibrosis: Bilateral upper lobe fibrosis, may cavitate, can be colonized by Aspergillus.
- Restrictive Defect: Costovertebral joint fusion → reduced chest expansion → reduced vital capacity.
Gastrointestinal
- Subclinical IBD: Colonoscopy shows microscopic gut inflammation in 30-50% without GI symptoms.
- Clinical IBD: 5-10% develop Crohn's disease or ulcerative colitis.
Renal
- IgA Nephropathy: 5-10%, usually asymptomatic microscopic haematuria.
- AA Amyloidosis: Rare complication of chronic inflammation → nephrotic syndrome, renal failure.
Neurological
- Cauda Equina Syndrome: Rare (less than 1%), late complication from dural ectasia or arachnoiditis, not disc prolapse.
- Spinal Cord Injury: Secondary to fracture or atlanto-axial subluxation. [18]
Signs
Spinal Examination
Inspection:
- Loss of lumbar lordosis (flattening)
- Increased thoracic kyphosis
- Cervical hyperextension (compensation)
- "Question mark" posture in severe disease
Palpation:
- Sacroiliac joint tenderness
- Spinous process tenderness
- Paraspinal muscle spasm
Movement Assessment:
1. Schober's Test (Lumbar Flexion)
- Patient standing, locate posterior superior iliac spines (PSIS—"dimples of Venus").
- Mark point at L5 level (line joining PSIS).
- Mark second point 10cm superior.
- Patient flexes forward maximally.
- Measure distance between marks.
- Normal: ≥15cm (≥5cm increase).
- Reduced (less than 5cm increase): Suggests reduced lumbar flexion.
- Modified Schober's: 5cm below and 10cm above (should increase to > 20cm).
2. Lateral Spinal Flexion
- Patient standing with hands by sides.
- Bend laterally, sliding hand down leg.
- Measure fingertip-to-floor distance.
- Normal: > 10cm movement; Reduced in AS.
3. Cervical Rotation
- Patient seated, examiner behind.
- Measure degrees of rotation.
- Normal: 70-80°; Reduced in AS.
4. Tragus-to-Wall Distance
- Patient stands with back to wall, heels touching wall.
- Measure distance from tragus to wall.
- Normal: less than 15cm; Increased indicates cervical kyphosis.
5. Occiput-to-Wall Distance
- Patient as above, attempting to touch occiput to wall.
- Normal: 0cm; Increased in thoracic kyphosis.
6. Chest Expansion
- Measure chest circumference at 4th intercostal space (nipple line).
- Measure at maximal expiration and maximal inspiration.
- Normal: > 5cm; Reduced (less than 2.5cm) from costovertebral joint involvement.
Special Tests
FABER Test (Patrick's Test)
- Flexion, ABduction, External Rotation of hip.
- Examiner applies downward pressure on flexed knee.
- Positive: Reproduces sacroiliac or hip pain.
Gaenslen's Test
- Patient supine, one hip flexed to chest, other leg hanging off table edge.
- Positive: Sacroiliac pain with hyperextension.
Sacroiliac Compression Test
- Patient lateral position.
- Examiner applies downward pressure on iliac crest.
- Positive: Sacroiliac pain.
Bath Metrology Indices
BASMI (Bath Ankylosing Spondylitis Metrology Index) Composite score (0-10) from:
- Cervical rotation
- Tragus-to-wall distance
- Lumbar flexion (Schober's)
- Lumbar side flexion
- Intermalleolar distance
5. Investigations
Laboratory Tests
Inflammatory Markers
- ESR and CRP: Elevated in 50-70% of active disease, but may be normal. Level correlates poorly with symptoms but useful for monitoring treatment response. [19]
- Full Blood Count: Anaemia of chronic disease in active inflammation.
Genetic Testing
- HLA-B27: Positive in 85-95% of AS patients.
- Sensitivity: 85-95% (high)
- Specificity: Low (only 1-5% of HLA-B27+ individuals develop AS)
- Utility: Supportive when clinical suspicion exists; not diagnostic alone; helps risk-stratify.
- When to Test: Young patient with inflammatory back pain and/or sacroiliitis on imaging.
- Not Recommended: Routine screening of HLA-B27 in general population or in asymptomatic relatives.
Seronegative Profile
- Rheumatoid Factor (RF): Negative (distinguishes from rheumatoid arthritis).
- Anti-CCP: Negative.
- ANA: Usually negative; low titre positivity can occur but high titre suggests alternative diagnosis.
Other Tests
- Renal Function: Screen for IgA nephropathy, amyloidosis.
- Urinalysis: Microscopic haematuria (IgA nephropathy).
- TB Screening: Before initiating biologic therapy (QuantiFERON/T-SPOT, CXR).
- Hepatitis B/C: Screen before biologics.
Imaging
Plain Radiography
Pelvis (AP View) - Sacroiliac Joints
New York Grading of Sacroiliitis (0-4):
- Grade 0: Normal
- Grade 1: Suspicious changes
- Grade 2: Minimal abnormality (small localized erosions, sclerosis)
- Grade 3: Moderate abnormality (erosions, sclerosis, widening/narrowing, partial ankylosis)
- Grade 4: Complete ankylosis (fusion)
Modified New York Criteria for AS require:
- Bilateral Grade ≥2 OR Unilateral Grade ≥3 PLUS ≥1 clinical criterion (IBP, limitation, reduced chest expansion).
Radiographic Evolution:
- Early: Blurring of subchondral bone plate, pseudo-widening
- Active: Erosions (irregular joint margins), subchondral sclerosis
- Late: Joint space narrowing, ankylosis (fusion)
Limitation: Changes take 7-10 years to develop; normal X-ray does not exclude early disease.
Spine (AP and Lateral)
Early Changes:
- Romanus Lesion ("Shiny Corner"): Erosion with reactive sclerosis at vertebral corners (anterosuperior, anteroinferior).
- Squaring of Vertebrae: Loss of normal anterior concavity; vertebral body becomes rectangular.
- Andersson Lesion: Destructive discovertebral lesion mimicking infection (pseudoarthrosis).
Progressive Changes:
- Syndesmophytes: Vertical ossification bridging vertebral bodies, originating from vertebral corners, following course of outer annulus fibrosus.
- vs DISH: DISH has flowing anterior ossification > 4 levels, disc spaces preserved, starts away from disc margin.
- vs Osteophytes: Osteophytes are horizontal, arise from vertebral body margin.
- "Dagger Sign": Ossification of supraspinous and interspinous ligaments creating central vertical density on AP view.
- Facet Joint Fusion: Ankylosis of apophyseal joints.
- "Bamboo Spine": Complete fusion creating smooth continuous outline.
- "Trolley Track Sign": Bilateral syndesmophytes on AP view.
Cervical Spine:
- Atlanto-axial subluxation (rare, less than 2%).
- Fusion in flexion → inability to visualize airway on lateral X-ray.
Magnetic Resonance Imaging (MRI)
Sequence: STIR (Short Tau Inversion Recovery) or T2 fat-suppressed sequences.
Sacroiliac Joints:
- Active Inflammation: Bone marrow edema (BME) in subchondral bone, high signal on STIR.
- Structural Changes: Erosions, sclerosis, fat metaplasia, ankylosis on T1.
- ASAS Definition of Positive MRI: BME highly suggestive of sacroiliitis associated with SpA if either:
- ≥2 lesions on single slice, OR
- ≥1 lesion on ≥2 consecutive slices.
Spine:
- Spondylitis: Vertebral corner edema (Romanus lesions on MRI).
- Spondylodiscitis: Discovertebral junction inflammation (Andersson lesion).
- Enthesitis: Inflammation at ligament attachments.
Advantages of MRI:
- Detects inflammation years before radiographic changes.
- Allows diagnosis of non-radiographic axial SpA (nr-axSpA).
- Monitors disease activity and treatment response.
- Disadvantage: Expensive, not universally available. [20]
Computed Tomography (CT)
Indications:
- Suspected Fracture: Mandatory in AS patient with trauma and pain; superior to X-ray.
- Pre-operative Planning: Spinal deformity correction surgery.
- Equivocal X-ray Findings: Better visualization of sacroiliac joints than X-ray.
Not Routine: Higher radiation; MRI preferred for inflammation.
Ultrasound
Use: Assess peripheral enthesitis (Achilles, plantar fascia). Findings: Thickening, hypoechogenicity, erosions, power Doppler signal.
Bone Densitometry (DEXA)
Indication: Screen for osteoporosis in established AS. Finding: 25-50% have low bone mineral density; increased fracture risk even with minor trauma.
Assessment Scores
BASDAI (Bath Ankylosing Spondylitis Disease Activity Index)
Six Questions (0-10 scale for each):
- Fatigue/tiredness
- Spinal pain
- Peripheral joint pain/swelling
- Enthesitis
- Morning stiffness severity
- Morning stiffness duration
Score: [Sum Q1-4 + Mean(Q5,Q6)] / 5 Interpretation:
- ≥4: Active disease (threshold for biologic therapy).
- Reduction ≥50% or ≥2 points: Clinically significant improvement (ASAS criteria).
ASDAS (Ankylosing Spondylitis Disease Activity Score)
Incorporates:
- Patient-reported outcomes (back pain, morning stiffness, patient global, peripheral pain/swelling)
- CRP or ESR
Interpretation:
- less than 1.3: Inactive disease
- 1.3-2.0: Low activity
- 2.1-3.5: High activity
- > 3.5: Very high activity
Advantage: More sensitive than BASDAI; includes objective marker (CRP).
BASFI (Bath Ankylosing Spondylitis Functional Index)
Ten Questions: Daily activities (dressing, bending, reaching, etc.). Score: 0-10; higher = worse function.
6. Diagnosis and Classification
ASAS Classification Criteria (2009)
For Axial Spondyloarthritis in patients with:
- Chronic back pain (≥3 months)
- Age of onset less than 45 years
Two Arms:
Imaging Arm:
- Sacroiliitis on imaging (X-ray or MRI) PLUS
- ≥1 SpA feature
Clinical Arm:
- HLA-B27 positive PLUS
- ≥2 SpA features
SpA Features:
- Inflammatory back pain
- Arthritis
- Enthesitis (heel)
- Uveitis
- Dactylitis
- Psoriasis
- Crohn's/colitis
- Good response to NSAIDs
- Family history of SpA
- HLA-B27 positive
- Elevated CRP
Sensitivity: 82.9%; Specificity: 84.4% [21]
Radiographic vs Non-Radiographic axSpA
Radiographic axSpA (r-axSpA = Ankylosing Spondylitis):
- Definite radiographic sacroiliitis (Modified New York criteria).
Non-Radiographic axSpA (nr-axSpA):
- Meets ASAS criteria but lacks definite radiographic sacroiliitis.
- May have MRI inflammation.
- Represents earlier disease or less severe phenotype.
- ~10-20% progress to r-axSpA over 2 years. [22]
Differential Diagnosis
Mechanical Back Pain
- Age > 45, acute onset, no morning stiffness, worse with activity, better with rest, localized.
Diffuse Idiopathic Skeletal Hyperostosis (DISH)
- Age > 50, flowing anterior ossification ≥4 levels, preserved disc spaces, no sacroiliitis, asymptomatic or mild.
Psoriatic Arthritis (Axial)
- Psoriasis, asymmetric sacroiliitis, chunky non-marginal syndesmophytes, peripheral arthritis.
Reactive Arthritis
- Preceding infection (GI/GU), acute onset, asymmetric oligoarthritis, urethritis, conjunctivitis.
Inflammatory Bowel Disease-Associated Arthritis
- Known IBD, peripheral arthritis, sacroiliitis (often asymptomatic).
Septic Sacroiliitis
- Unilateral, acute onset, fever, elevated WCC/CRP, IV drug use, immunosuppression.
Malignancy
- Age > 50, progressive pain, night pain, weight loss, systemic symptoms, focal lesions.
7. Management
Principles
- Early Diagnosis and Treatment: Reduce irreversible structural damage.
- Multidisciplinary Approach: Rheumatology, physiotherapy, occupational therapy, ophthalmology, orthopaedics.
- Treat to Target: Aim for inactive disease (ASDAS less than 1.3) or low disease activity (ASDAS less than 2.1).
- Lifelong Management: Chronic condition requiring ongoing monitoring and treatment adjustment.
Non-Pharmacological
Physiotherapy and Exercise
CRITICAL INTERVENTION - equivalent importance to medication.
Benefits:
- Maintains spinal mobility and chest expansion.
- Reduces pain and stiffness.
- Improves posture and function.
- Slows radiographic progression (evidence from observational studies).
Recommendations:
- Frequency: Daily home exercises plus supervised physiotherapy.
- Type:
- Stretching: Spinal extension, hip flexor stretches.
- Strengthening: Core, paraspinal muscles, shoulder girdle.
- Aerobic: Swimming (excellent—extension exercises in water), cycling, walking.
- Breathing exercises: Maintain chest expansion.
- Group Programs: Improve adherence and outcomes vs individual.
- Avoid: Contact sports (fracture risk in fused spine). [23]
Posture and Lifestyle
- Sleep: Firm mattress, single pillow or no pillow (avoid multiple pillows promoting cervical flexion).
- Work: Ergonomic workstation, frequent breaks from prolonged sitting/standing.
- Driving: Ensure adequate neck mobility; consider extended mirrors if cervical rotation limited.
Smoking Cessation
- MANDATORY: Smoking associated with:
- Increased disease activity
- Accelerated radiographic progression
- Worse functional outcomes
- Poorer response to TNF inhibitors
- Smoking cessation should be reinforced at every visit. [24]
Pharmacological
NSAIDs (First-Line)
Evidence: NSAIDs provide significant symptom relief; continuous use may slow radiographic progression. [25]
Recommendations:
- Initial Choice: Any NSAID; individualize based on response and side effects.
- Examples:
- Naproxen 500mg BD
- Diclofenac 50mg TDS or 75mg BD
- Etoricoxib 90mg OD (COX-2 selective)
- Dosing: Full anti-inflammatory dose (not PRN); continuous daily use preferred.
- Duration: Trial for 2-4 weeks at maximal tolerated dose before switching.
- If Inadequate Response: Try alternative NSAID (individual variation in response).
Contraindications/Cautions:
- Peptic ulcer disease, GI bleeding (co-prescribe PPI).
- Renal impairment.
- Cardiovascular disease (COX-2 inhibitors increase CV risk).
- Pregnancy.
Conventional DMARDs
Sulfasalazine
- Indication: Peripheral arthritis in axSpA.
- Dose: 2-3g daily (build up gradually).
- Evidence: Effective for peripheral joints; NO effect on axial disease or radiographic progression.
- Use in AS: Limited to patients with peripheral manifestations.
Methotrexate
- Evidence: NOT effective for axial disease in AS.
- Use: Consider only if significant peripheral arthritis unresponsive to sulfasalazine.
Conclusion: Conventional DMARDs (MTX, SSZ, LEF) are ineffective for axial disease and should not be used for this indication.
Glucocorticoids
- Systemic: NOT routinely recommended for axial disease; minimal efficacy, significant side effects.
- Intra-articular: Useful for peripheral arthritis or enthesitis (e.g., sacroiliac joint injection under imaging).
- Topical (Eye): First-line for anterior uveitis (ophthalmology-directed).
Biologic Therapies
TNF Inhibitors (TNFi)
Five Agents Licensed:
- Adalimumab (Humira): SC 40mg every 2 weeks
- Etanercept (Enbrel): SC 50mg weekly
- Infliximab (Remicade): IV 5mg/kg at 0, 2, 6 weeks, then every 6-8 weeks
- Golimumab (Simponi): SC 50mg monthly
- Certolizumab Pegol (Cimzia): SC 200mg every 2 weeks or 400mg monthly
Evidence:
- Efficacy: 50-60% achieve ASAS40 response (≥40% improvement). [7]
- Onset: Rapid, often within 2-4 weeks.
- Radiographic Progression: May slow syndesmophyte formation; data conflicting, benefit most evident when initiated early.
- Extra-articular: Effective for IBD (adalimumab, infliximab), uveitis response variable.
NICE/ASAS Criteria for TNFi:
- Diagnosis confirmed by rheumatologist (ASAS criteria).
- High disease activity: BASDAI ≥4 on two occasions ≥4 weeks apart.
- Failed NSAIDs: Inadequate response to ≥2 NSAIDs at maximal dose for ≥4 weeks (or contraindicated/intolerant).
- Spinal symptoms: Limitation of spinal movement (Schober's less than 5cm or lumbar side flexion less than 10cm).
Response Assessment:
- Review at 12 weeks.
- Continue if: BASDAI improves ≥50% OR absolute decrease ≥2 points.
- Stop if: Inadequate response.
Switching TNFi: ~50% of non-responders to first TNFi respond to second TNFi.
IL-17 Inhibitors
Agents:
- Secukinumab (Cosentyx): SC 150mg weekly x5, then monthly
- Ixekizumab (Taltz): SC 160mg loading, then 80mg every 2-4 weeks
Evidence:
- Efficacy: Similar to TNFi; ASAS40 response ~50%. [8]
- Advantages: Effective in TNFi non-responders; superior for psoriatic arthritis.
- Disadvantages: May worsen IBD (use with caution if co-existing Crohn's/UC); increased Candida infections.
Indications:
- TNFi inadequate response or intolerance.
- Concomitant psoriasis (preferred).
- Contraindication to TNFi.
JAK Inhibitors
Agent: Tofacitinib (not widely licensed for AS; some evidence in trials).
Other Agents (Not Recommended):
- IL-12/23 inhibitors (ustekinumab): NOT effective for axial SpA.
- Rituximab, abatacept: NOT effective.
Pre-Biologic Screening
Mandatory:
- Tuberculosis: QuantiFERON/T-SPOT, CXR; treat latent TB before starting biologic.
- Hepatitis B/C: Screen; manage active infection before/during treatment.
- HIV: Screen (biologics not absolutely contraindicated but increased risk).
- Vaccinations: Update pneumococcal, influenza; avoid live vaccines once on biologic.
- Pregnancy Planning: Discuss contraception; some biologics compatible with pregnancy/breastfeeding.
Contraindications:
- Active infection (including chronic infections like TB, HBV).
- Severe heart failure (NYHA III/IV for TNFi).
- Demyelinating disease (TNFi).
- Malignancy (within 5 years, excluding non-melanoma skin cancer).
Surgical
Indications
1. Spinal Fracture (Emergency)
- Chalk Stick Fracture: High-energy (by AS standards) unstable fracture.
- Management:
- Immediate immobilization (avoid flexion/extension).
- CT whole spine (high incidence of non-contiguous fractures).
- Neurosurgical/spinal orthopaedic consultation.
- Surgery: Long-segment fixation (≥2 levels above and below); anterior and posterior stabilization often required.
- Outcome: High morbidity/mortality (10-30% mortality if cervical fracture with cord injury). [9]
2. Spinal Deformity Correction
- Indication: Severe fixed kyphosis causing:
- Inability to see horizon (chin-on-chest deformity).
- Functional impairment (cannot stand erect, affects swallowing).
- Respiratory compromise.
- Procedure: Pedicle Subtraction Osteotomy (PSO) or Smith-Petersen Osteotomy (SPO).
- PSO: Vertebral wedge resection (usually L2/L3), closing wedge, corrects 30-40° kyphosis.
- Risks: High morbidity (neurological injury 10-30%, significant blood loss, prolonged surgery).
- Outcome: Dramatic improvement in quality of life for selected patients. [26]
3. Hip Arthroplasty
- Indication: Severe hip involvement with ankylosis or advanced arthritis.
- Prevalence: 25-30% of AS patients develop hip involvement; 5-10% require arthroplasty.
- Timing: Perform before hip fuses completely (better outcomes with preserved mobility).
- Technical Considerations: Fused spine makes positioning difficult; risk of heterotopic ossification (use prophylaxis).
4. Atlantoaxial Stabilization
- Indication: Rare atlanto-axial subluxation with cord compression.
Monitoring
Baseline:
- BASDAI, BASFI, ASDAS
- ESR, CRP, FBC, LFTs, renal function
- X-ray pelvis, spine
- Consider MRI SI joints (establish inflammation)
- DEXA scan
- Ophthalmology review if uveitis
- Cardiology if murmur/symptoms
- Chest X-ray
Follow-Up (Stable on Treatment):
- 3-6 Monthly: Clinical review, BASDAI/ASDAS, ESR/CRP.
- Annually: BASFI, metrology (Schober's, chest expansion, occiput-to-wall).
- Every 2 Years: X-ray pelvis/spine (assess progression).
- On Biologics: FBC, LFTs, CRP every 3 months initially, then 6-monthly.
Treatment Escalation Triggers:
- BASDAI ≥4 despite NSAIDs → consider biologic.
- Inadequate response to first biologic at 12 weeks → switch biologic.
- Disease flare on stable treatment → optimize dose, switch agent.
8. Complications
Spinal Fractures
"Chalk Stick Fracture" - Most feared complication. [5,6,9]
Mechanism:
- Fused spine = long lever arm, no shock absorption.
- Osteoporosis from immobility and inflammation.
- Minor trauma (fall from standing, sudden deceleration in vehicle) creates three-column fracture (unstable).
Presentation:
- New onset or increased back/neck pain after trauma (even minor).
- Neurological deficit (50% have cord injury).
Diagnosis:
- High Index of Suspicion: Any trauma in AS patient = CT whole spine.
- Plain X-ray: Misses 30% (obscured by syndesmophytes, deformity).
- CT: Gold standard.
- MRI: If neurological deficit (assess cord compression, hematoma).
Management:
- Immobilization: Rigid collar (cervical), bed rest (thoracolumbar).
- Surgery: Long-segment fixation (≥2 levels above/below), often combined anterior-posterior approach.
- Non-operative: Only if neurologically intact, stable fracture (rare).
Prognosis:
- Mortality: 10-30% (cervical fractures with cord injury).
- Permanent neurological deficit: 30-50%.
Cauda Equina Syndrome
Rare (less than 1%) late complication, distinct from typical lumbar disc CES. [18]
Pathophysiology:
- Dural Ectasia: Chronic arachnoiditis → dural sac erosion → widening, diverticula.
- Arachnoid Cysts: Compression of cauda equina nerve roots.
Presentation:
- Insidious onset (unlike acute disc CES).
- Lower limb weakness, sensory loss (saddle anesthesia), bladder/bowel dysfunction.
- Occurs 20-30 years after AS diagnosis.
Diagnosis:
- MRI: Widened dural sac, erosion of posterior vertebral elements, arachnoid cysts, nerve root clumping.
Management:
- Conservative: Symptom management (often progressive).
- Surgery: Cyst drainage, shunting (variable outcomes).
Cardiovascular
Aortitis and Aortic Regurgitation (2-10%)
- Chronic inflammation → aortic root fibrosis → dilation → AR.
- Typically develops > 15 years after diagnosis.
- Clinical: Early diastolic murmur, bounding pulse, heart failure symptoms.
- Diagnosis: Echocardiography.
- Management: Standard AR management; valve replacement if severe.
Conduction Defects (1-3%)
- AV block (1st, 2nd, 3rd degree), bundle branch block.
- May require pacemaker.
Increased Cardiovascular Risk
- Chronic inflammation → accelerated atherosclerosis.
- Relative risk of MI ~1.5-2x general population.
- Manage CV risk factors aggressively (statin, BP control).
Pulmonary
Apical Lung Fibrosis (1-2%)
- Bilateral upper lobe fibrosis; may cavitate.
- Colonization with Aspergillus (aspergilloma) or atypical mycobacteria.
- Often asymptomatic; may cause hemoptysis if aspergilloma.
Restrictive Lung Disease
- Costovertebral joint fusion → reduced chest expansion → reduced vital capacity.
- Usually mild; compensated by diaphragmatic breathing.
- Exacerbated by kyphosis (compresses thorax).
Renal
IgA Nephropathy (5-10%)
- Usually asymptomatic; detected on urinalysis (microscopic hematuria, proteinuria).
- Rarely progresses to renal failure.
AA Amyloidosis (Rare)
- Complication of chronic inflammation (if poorly controlled).
- Presents with nephrotic syndrome, renal failure.
- Diagnosis: Renal biopsy (Congo red staining).
- Management: Control inflammation (biologics), supportive.
Osteoporosis
Prevalence: 25-50% of AS patients have low bone mineral density.
Mechanisms:
- Chronic inflammation (TNF-α, IL-6 → osteoclast activation).
- Immobility.
- Glucocorticoid use (if applicable).
Consequences:
- Vertebral compression fractures (can occur without trauma).
- Increased fracture risk even with minor trauma.
Management:
- Screening: DEXA scan at diagnosis, repeat every 2-5 years.
- Treatment: Calcium/Vitamin D, bisphosphonates if T-score ≤ -2.5 or fragility fracture.
Atlanto-Axial Subluxation
Rare (less than 2%) but catastrophic.
- Occurs with cervical spine involvement.
- Presentation: Myelopathy (upper motor neuron signs), respiratory compromise (high cord compression).
- Diagnosis: Flexion/extension cervical X-ray, MRI.
- Management: Surgical fusion (C1-C2).
9. Prognosis
Disease Course
Variable Natural History:
- 25%: Mild disease, minimal progression, good function.
- 50%: Moderate disease, intermittent flares, some limitation, usually maintain independence.
- 25%: Severe disease, progressive spinal fusion, significant disability.
Predictors of Poor Prognosis
- Hip Involvement: Strongest predictor of severe disease and need for arthroplasty.
- Young Age at Onset: less than 20 years associated with worse outcomes.
- Elevated CRP: Persistent elevation correlates with radiographic progression.
- Smoking: Accelerates disease, reduces treatment response.
- Poor Response to NSAIDs: Suggests more aggressive disease.
- HLA-B27 Positive: Some studies suggest faster progression (conflicting data).
- Baseline Radiographic Damage: Existing syndesmophytes predict further progression. [13]
Functional Outcomes
Pre-Biologic Era:
- 50% work disability by 15 years.
- 30-40% significant functional limitation by 20 years.
Biologic Era:
- Improved function and quality of life.
- Uncertain if radiographic progression truly slowed (data conflicting).
- Early treatment may prevent irreversible damage.
Mortality
Increased Mortality Risk: 1.5-2x general population.
Causes:
- Cardiovascular disease (most common).
- Respiratory disease (apical fibrosis, restrictive defect).
- Spinal fractures and neurological complications.
- Infections (increased with immunosuppression).
- Amyloidosis (rare).
Life Expectancy: Reduced by ~5 years on average (improved in modern era with biologics).
10. Special Situations
Pregnancy
Fertility: Not affected by AS itself.
Disease Activity:
- Variable; some improve, some worsen.
- Mechanical back pain common in third trimester (lumbar lordosis).
Medications:
- Safe: Sulfasalazine, hydroxychloroquine, azathioprine (if needed).
- Avoid: Methotrexate (teratogenic), NSAIDs (first trimester and third trimester > 32 weeks).
- Biologics:
- TNFi: Certolizumab pegol (no placental transfer) preferred. Adalimumab, etanercept, infliximab cross placenta but limited data suggests safe; stop third trimester.
- IL-17i: Limited data; avoid if possible.
Delivery:
- Vaginal delivery usually possible if hips mobile.
- Epidural: May be difficult/impossible if spinal fusion; early anesthetic consultation.
- Cesarean section: If fused hips prevent lithotomy position.
Anaesthesia
Critical Considerations:
Airway:
- Fused cervical spine in flexion → difficult/impossible laryngoscopy.
- Awake fibreoptic intubation often required.
- Pre-operative assessment and planning essential.
Positioning:
- Limited hip/spine movement → positioning challenges.
- Padding required (bony prominences).
Regional Anaesthesia:
- Epidural/spinal: Difficult or impossible with fused spine.
- Early consultation with anaesthetics for elective procedures.
Post-operative:
- Respiratory complications (restrictive defect, reduced cough).
- Early mobilization critical (prevent VTE, maintain function).
Juvenile-Onset AS
Definition: Symptom onset less than 16 years.
Features:
- More likely to present with peripheral arthritis (70% vs 30% in adults).
- Hip involvement common (worse prognosis).
- Delayed diagnosis (atypical presentation).
Management:
- Similar to adult AS.
- Biologics effective and safe in children (approved from age 6).
- MDT approach including pediatric rheumatology.
11. Patient Education
What is Ankylosing Spondylitis?
Ankylosing Spondylitis (AS) is a type of arthritis that primarily affects your spine and the joints where your spine connects to your pelvis (sacroiliac joints). "Ankylosing" means stiffening or fusing, and "spondylitis" means inflammation of the spine.
In AS, your immune system mistakenly attacks the joints and ligaments of your spine, causing inflammation and pain. Over time, as your body tries to heal this inflammation, new bone can form, which may eventually cause parts of your spine to fuse together. This fusion reduces flexibility and can lead to a hunched posture.
What Causes It?
The exact cause is unknown, but genetics play a major role. Most people with AS (about 90%) have a gene called HLA-B27. However, having this gene doesn't mean you'll definitely get AS—only about 1-5% of people with HLA-B27 develop the condition. Environmental factors (possibly infections) may trigger AS in genetically susceptible people.
Will I End Up in a Wheelchair?
No. Most people with AS do not become severely disabled, especially with modern treatments. While the disease varies from person to person:
- 25% have mild disease with minimal impact.
- 50% have moderate disease with some limitations but maintain independence.
- 25% have more severe disease, but even these individuals often remain mobile with proper treatment and physiotherapy.
The key is early diagnosis, treatment, and staying active.
Treatment Options
1. Exercise and Physiotherapy (Most Important)
- Exercise is as important as medication—it keeps your spine flexible and strong.
- Recommended: Daily stretching, swimming (excellent), yoga, Pilates.
- Group exercise programs designed for AS patients are very helpful.
2. Medications
- Anti-inflammatory drugs (NSAIDs): First-line treatment (e.g., naproxen, ibuprofen). Take regularly, not just when painful.
- Biologic therapies: If NSAIDs don't control symptoms, powerful injectable medications (TNF inhibitors, IL-17 inhibitors) can dramatically reduce inflammation. These are highly effective for most patients.
3. Lifestyle
- Don't smoke: Smoking makes AS worse and accelerates spinal fusion.
- Sleep posture: Firm mattress, one pillow (or none) to avoid neck flexion.
- Stay active: Avoid prolonged sitting; take movement breaks.
Will I Be Able to Work?
Yes, most people with AS continue working. You may need workplace modifications:
- Adjustable desk/chair.
- Frequent breaks to move.
- Flexible hours for morning stiffness.
In the UK, you're protected under the Equality Act—employers must make reasonable adjustments.
Can I Have Children?
Yes. AS doesn't affect fertility. Women with AS can have normal pregnancies, though you'll need to discuss medications with your rheumatologist (some are safe, others need to be stopped). Delivery is usually normal, but if your hips are affected, discuss with your obstetrician.
There's a genetic component: if you have AS and are HLA-B27 positive, each child has ~50% chance of inheriting HLA-B27, but only ~5-10% chance of developing AS.
Red Flags—When to Seek Urgent Help
- Red, painful eye with light sensitivity: Possible uveitis—see ophthalmology urgently (same day).
- New back/neck pain after a fall or accident: Even minor trauma can cause serious fractures—go to A&E.
- Numbness in saddle area, difficulty urinating, leg weakness: Rare nerve compression—emergency.
- New chest pain or severe shortness of breath: Could be heart/lung complication—seek medical help.
Support and Resources
- National Ankylosing Spondylitis Society (NASS): UK charity providing information, support groups, exercise programs (www.nass.co.uk).
- Arthritis Research UK: Information and resources.
- Local physiotherapy: Ask your rheumatologist for referral to specialist AS physio.
12. Examination Focus (Viva Vault)
Core Questions
Q1: What is Ankylosing Spondylitis and how does it differ from other spondyloarthropathies?
Model Answer: Ankylosing Spondylitis is a chronic inflammatory spondyloarthropathy characterized by axial skeleton inflammation, particularly sacroiliitis and spondylitis, leading to progressive ossification and spinal fusion. It is the prototypic axial spondyloarthropathy and represents the radiographic end of the axial SpA spectrum.
It differs from other spondyloarthropathies in having predominant axial involvement (spine and sacroiliac joints), whereas psoriatic arthritis, reactive arthritis, and enteropathic arthritis more commonly present with peripheral arthritis. AS has the highest association with HLA-B27 (85-95%) and the strongest genetic component. Radiographically, AS produces characteristic marginal syndesmophytes (vertical), unlike the chunky non-marginal syndesmophytes of psoriatic arthritis or the flowing ossification of DISH.
Q2: Describe the pathophysiology of syndesmophyte formation.
Model Answer: Syndesmophyte formation occurs through a sequence:
- Enthesitis: Primary lesion is inflammation at the enthesis—where the outer fibers of the annulus fibrosus insert into the vertebral corner (Sharpey's fibers).
- Erosion: Inflammatory cells (T cells, macrophages) driven by TNF-α and IL-17 cause erosion of the vertebral corner, creating Romanus lesions (seen as bone marrow edema on MRI, sclerosis on X-ray—"shiny corners").
- Osteoproliferation: Paradoxically, the same inflammatory milieu triggers new bone formation via BMP and Wnt signaling pathways. Osteoblasts deposit new bone along the path of the outer annulus fibers.
- Syndesmophyte: Vertical bony bridge forms between adjacent vertebral bodies, originating from the vertebral corner and following the course of the annulus (marginal).
- Ankylosis: With time, syndesmophytes from adjacent levels join, creating continuous fusion—the "bamboo spine."
This process is mechanically driven (high-stress sites) and inflammation-mediated (cytokine environment).
Q3: What are the ASAS classification criteria for axial spondyloarthritis?
Model Answer: The ASAS criteria (2009) classify axial SpA in patients with chronic back pain ≥3 months and onset less than 45 years. There are two arms:
Imaging Arm:
- Sacroiliitis on imaging (X-ray: bilateral grade ≥2 or unilateral grade ≥3; OR MRI: active inflammation) PLUS
- ≥1 SpA feature.
Clinical Arm:
- HLA-B27 positive PLUS
- ≥2 SpA features.
SpA features include: Inflammatory back pain, arthritis, enthesitis (heel), uveitis, dactylitis, psoriasis, IBD, good response to NSAIDs, family history of SpA, HLA-B27, elevated CRP.
Sensitivity 82.9%, Specificity 84.4%—these are classification criteria for research, but guide clinical diagnosis.
Q4: Explain the "Chalk Stick Fracture" and its management.
Model Answer: The "chalk stick fracture" describes fractures occurring in the ankylosed AS spine. The fused spine acts as a long, rigid lever with no shock absorption and is osteoporotic from chronic inflammation and immobility. Even minor trauma (fall from standing, sudden deceleration) can cause transverse three-column fractures, typically through the disc space or fused segment, which are highly unstable.
Presentation: Any trauma in an AS patient with new/worsened back or neck pain. High suspicion required as these are frequently missed.
Diagnosis:
- Imaging: CT whole spine is mandatory (X-ray misses 30% due to overlying ossification and deformity).
- Check for non-contiguous fractures (20% have multiple levels).
- MRI if neurological deficit (assess cord compression).
Management:
- Immediate immobilization in neutral position (avoid flexion/extension).
- Neurosurgical/spinal orthopaedic consultation.
- Surgical fixation: Long-segment (≥2 levels above/below), often combined anterior-posterior approach.
- High morbidity: 50% have neurological injury; 10-30% mortality with cervical fractures.
Q5: When would you start a biologic therapy in AS, and which would you choose?
Model Answer: Biologic therapy is indicated when:
- Diagnosis confirmed (meets ASAS criteria).
- High disease activity: BASDAI ≥4 on two occasions ≥4 weeks apart.
- Failed NSAIDs: Inadequate response to ≥2 different NSAIDs at maximal tolerated dose for ≥4 weeks each (or contraindicated/intolerant).
- Evidence of spinal limitation (Schober's less than 5cm or lateral flexion less than 10cm).
First-Line Biologic: TNF inhibitor—all five (adalimumab, etanercept, infliximab, golimumab, certolizumab) are effective with ~50-60% achieving ASAS40 response. Choice based on:
- Patient preference (SC vs IV, frequency).
- Comorbidities: If co-existing IBD, use adalimumab or infliximab (infliximab preferred for moderate-severe IBD).
- Pregnancy planning: Certolizumab pegol (no placental transfer).
Second-Line: If TNFi fails/intolerant, use IL-17 inhibitor (secukinumab or ixekizumab). ~50% of TNFi non-responders respond to IL-17i. Preferred if concomitant psoriasis. Caution if IBD (may worsen).
Response Assessment: Review at 12 weeks. Continue if BASDAI reduces ≥50% or ≥2 points absolute decrease. If inadequate, switch to alternative biologic.
Q6: What are the extra-articular manifestations of AS and their significance?
Model Answer: Extra-articular manifestations occur in 30-50% of AS patients:
1. Anterior Uveitis (25-30%)
- Most common; strongly HLA-B27 associated.
- Acute onset, unilateral, painful red eye, photophobia, blurred vision.
- Recurrent, alternating eyes, non-granulomatous.
- Significance: Requires urgent ophthalmology (same-day)—risk of permanent vision loss if untreated. Treated with topical corticosteroids.
2. Aortic Regurgitation (2-10%)
- Chronic aortitis → aortic root fibrosis and dilation → AR.
- Develops > 15 years after AS diagnosis.
- Significance: Progressive; may require valve replacement. All AS patients should have baseline and periodic echocardiography if murmur or symptoms.
3. Apical Lung Fibrosis (1-2%)
- Bilateral upper lobe fibrosis; may cavitate.
- Significance: Risk of Aspergillus colonization (aspergilloma) or atypical mycobacteria. May cause hemoptysis.
4. Inflammatory Bowel Disease (5-10%)
- Clinical Crohn's/UC; 30-50% have subclinical gut inflammation.
- Significance: Affects biologic choice (TNFi effective for both; IL-17i may worsen IBD).
5. Cardiac Conduction Defects (1-3%)
- AV blocks; may require pacemaker.
6. Renal: IgA Nephropathy (5-10%); AA Amyloidosis (rare).
7. Neurological: Cauda Equina Syndrome (less than 1%) from dural ectasia, not disc prolapse.
Significance: These manifestations increase morbidity, require multidisciplinary management (ophthalmology, cardiology, gastroenterology), and influence treatment choices.
Q7: How do you perform and interpret Schober's Test?
Model Answer: Schober's Test assesses lumbar spine flexion.
Technique:
- Patient standing erect, feet together.
- Locate posterior superior iliac spines (PSIS—"dimples of Venus"), which correspond to S2 level.
- Mark a point at the midline at the level of PSIS (approximately L5).
- Using a tape measure, mark a second point 10cm superior to the first mark.
- Ask the patient to flex forward maximally (touch toes), keeping knees straight.
- Measure the distance between the two marks.
Interpretation:
- Normal: Distance increases to ≥15cm (i.e., ≥5cm increase from baseline 10cm). This reflects normal lumbar flexion stretching the skin.
- Reduced (less than 5cm increase): Suggests reduced lumbar flexion, consistent with AS or other causes of spinal stiffness.
Modified Schober's: Mark 5cm below and 10cm above PSIS (15cm baseline); should increase to ≥20cm (≥5cm increase).
Limitations: Operator-dependent; affected by hip flexion (can compensate for reduced lumbar movement); not specific to AS.
Clinical Use: Part of BASMI score; monitors disease progression; supports diagnosis in context.
13. References
- Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73-84. doi:10.1016/S0140-6736(16)31591-4
- Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379-1390. doi:10.1016/S0140-6736(07)60635-7
- Brown MA, Kenna T, Wordsworth BP. Genetics of ankylosing spondylitis—insights into pathogenesis. Nat Rev Rheumatol. 2016;12(2):81-91. doi:10.1038/nrrheum.2015.133
- Sieper J, van der Heijde D, Landewe R, et al. New criteria for inflammatory back pain in patients with chronic back pain: a real patient exercise by experts from the Assessment of SpondyloArthritis international Society (ASAS). Ann Rheum Dis. 2009;68(6):784-788. doi:10.1136/ard.2008.101501
- Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009;18(2):145-156. doi:10.1007/s00586-008-0764-0
- Caron T, Bransford R, Nguyen Q, et al. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010;35(11):E458-E464. doi:10.1097/BRS.0b013e3181cc764f
- van der Heijde D, Kivitz A, Schiff MH, et al. Efficacy and safety of adalimumab in patients with ankylosing spondylitis: results of a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2006;54(7):2136-2146. doi:10.1002/art.21913
- Baeten D, Sieper J, Braun J, et al. Secukinumab, an interleukin-17A inhibitor, in ankylosing spondylitis. N Engl J Med. 2015;373(26):2534-2548. doi:10.1056/NEJMoa1505066
- Thumbikat P, Hariharan RP, Ravichandran G, McClelland MR, Mathew KM. Spinal cord injury in patients with ankylosing spondylitis: a 10-year review. Spine (Phila Pa 1976). 2007;32(26):2989-2995. doi:10.1097/BRS.0b013e31815cd173
- Woodward LJ, Kam PC. Ankylosing spondylitis: recent developments and anaesthetic implications. Anaesthesia. 2009;64(5):540-548. doi:10.1111/j.1365-2044.2008.05838.x
- Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ. Global prevalence of ankylosing spondylitis. Rheumatology (Oxford). 2014;53(4):650-657. doi:10.1093/rheumatology/ket387
- Cortes A, Hadler J, Pointon JP, et al. Identification of multiple risk variants for ankylosing spondylitis through high-density genotyping of immune-related loci. Nat Genet. 2013;45(7):730-738. doi:10.1038/ng.2667
- Pradeep DJ, Keat AC, Gaffney K. Predicting outcome in ankylosing spondylitis. Rheumatology (Oxford). 2008;47(7):942-945. doi:10.1093/rheumatology/ken172
- Bowness P. HLA-B27. Annu Rev Immunol. 2015;33:29-48. doi:10.1146/annurev-immunol-032414-112110
- Schett G, Lories RJ, D'Agostino MA, et al. Enthesitis: from pathophysiology to treatment. Nat Rev Rheumatol. 2017;13(12):731-741. doi:10.1038/nrrheum.2017.188
- Appel H, Kuhne M, Spiekermann S, et al. Immunohistochemical analysis of hip arthritis in ankylosing spondylitis: evaluation of the bone-cartilage interface and subchondral bone marrow. Arthritis Rheum. 2006;54(6):1805-1813. doi:10.1002/art.21840
- Rosenbaum JT. Uveitis in spondyloarthritis including psoriatic arthritis, ankylosing spondylitis, and inflammatory bowel disease. Clin Rheumatol. 2015;34(6):999-1002. doi:10.1007/s10067-015-2960-8
- Ahn NU, Ahn UM, Nallamshetty L, et al. Cauda equina syndrome in ankylosing spondylitis (the CES-AS syndrome): meta-analysis of outcomes after medical and surgical treatments. J Spinal Disord. 2001;14(5):427-433. doi:10.1097/00002517-200110000-00009
- Spoorenberg A, van der Heijde D, de Klerk E, et al. Relative value of erythrocyte sedimentation rate and C-reactive protein in assessment of disease activity in ankylosing spondylitis. J Rheumatol. 1999;26(4):980-984.
- Rudwaleit M, Jurik AG, Hermann KG, et al. Defining active sacroiliitis on magnetic resonance imaging (MRI) for classification of axial spondyloarthritis: a consensual approach by the ASAS/OMERACT MRI group. Ann Rheum Dis. 2009;68(10):1520-1527. doi:10.1136/ard.2009.110767
- Rudwaleit M, van der Heijde D, Landewe R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68(6):777-783. doi:10.1136/ard.2009.108233
- Poddubnyy D, Rudwaleit M, Haibel H, et al. Rates and predictors of radiographic sacroiliitis progression over 2 years in patients with axial spondyloarthritis. Ann Rheum Dis. 2011;70(8):1369-1374. doi:10.1136/ard.2010.145995
- Dagfinrud H, Kvien TK, Hagen KB. Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev. 2008;(1):CD002822. doi:10.1002/14651858.CD002822.pub3
- Chung HY, Machado P, van der Heijde D, D'Agostino MA, Dougados M. Smokers in early axial spondyloarthritis have earlier disease onset, more disease activity, inflammation and damage, and poorer function and health-related quality of life: results from the DESIR cohort. Ann Rheum Dis. 2012;71(6):809-816. doi:10.1136/annrheumdis-2011-200180
- Wanders A, van der Heijde D, Landewe R, et al. Nonsteroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis Rheum. 2005;52(6):1756-1765. doi:10.1002/art.21054
- Qian BP, Qiu Y, Wang B, et al. Pedicle subtraction osteotomy through pseudarthrosis to correct thoracolumbar kyphotic deformity in advanced ankylosing spondylitis. Eur Spine J. 2012;21(4):711-718. doi:10.1007/s00586-011-2084-7
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Sacroiliac Joint Anatomy
- HLA System and Autoimmunity
Differentials
Competing diagnoses and look-alikes to compare.
- Mechanical Back Pain
- Psoriatic Arthritis
- Reactive Arthritis
- Inflammatory Bowel Disease-Associated Arthritis
- Diffuse Idiopathic Skeletal Hyperostosis (DISH)
Consequences
Complications and downstream problems to keep in mind.
- Spinal Fractures
- Anterior Uveitis
- Aortic Regurgitation
- Restrictive Lung Disease