Acute Cholecystitis
Acute cholecystitis is an acute inflammatory condition of the gallbladder, most commonly resulting from cystic duct obst... MRCS exam preparation.
What matters first
Acute cholecystitis is an acute inflammatory condition of the gallbladder, most commonly resulting from cystic duct obst... MRCS exam preparation.
Gangrenous cholecystitis - necrotic wall with perforation risk
9 Jan 2025
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Gangrenous cholecystitis - necrotic wall with perforation risk
- Perforation with biliary peritonitis
- Sepsis or septic shock
- Emphysematous cholecystitis - gas-forming organisms
Exam focus
Current exam surfaces linked to this topic.
- MRCS
Linked comparisons
Differentials and adjacent topics worth opening next.
- Acute Cholangitis
- Acute Pancreatitis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acute Cholecystitis
1. Clinical Overview
Definition and Importance
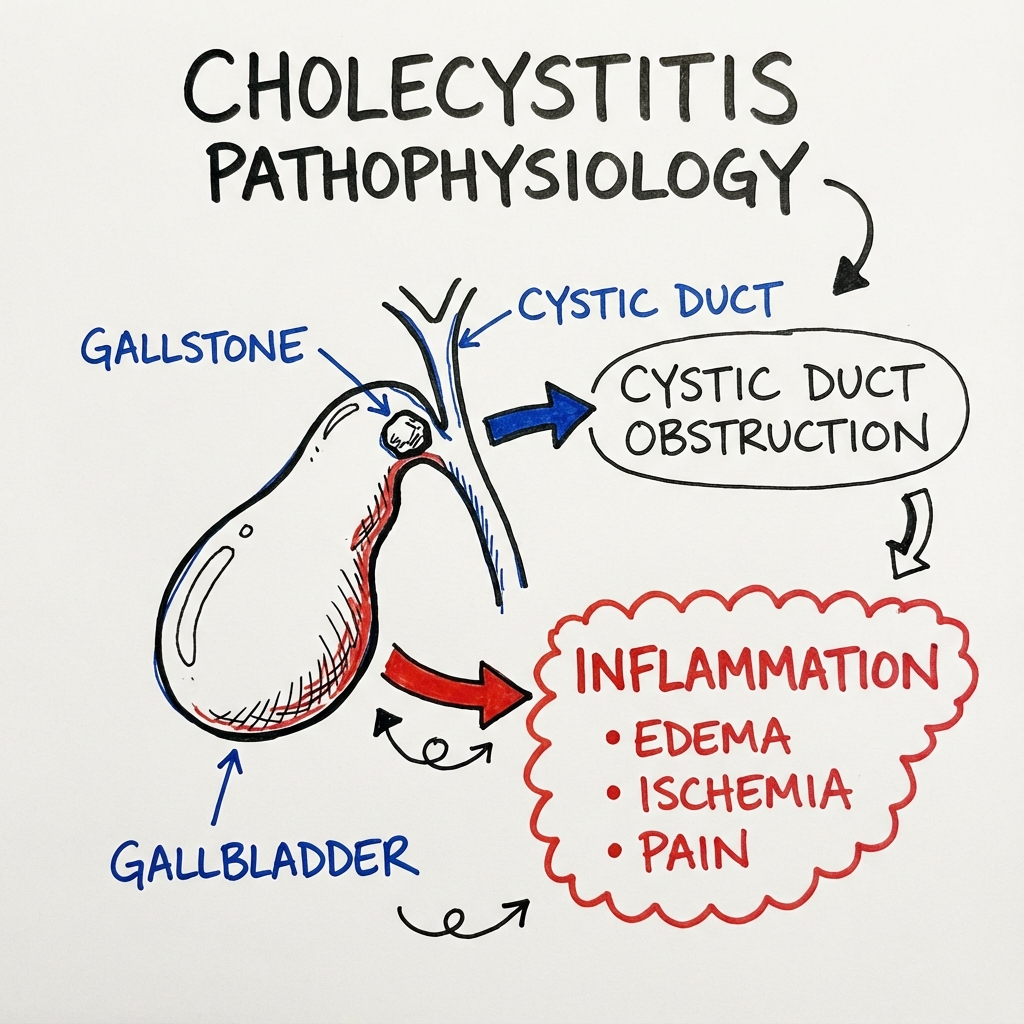
Acute cholecystitis is an acute inflammatory condition of the gallbladder, most commonly resulting from cystic duct obstruction by an impacted gallstone. This condition represents one of the most frequent indications for emergency abdominal surgery worldwide, with approximately 20% of patients with symptomatic gallstones developing acute cholecystitis during their lifetime.[1] The Tokyo Guidelines (TG18/TG21) provide internationally validated diagnostic criteria and severity grading that have standardised clinical practice and improved patient outcomes.[2,3]
The pathophysiological process involves gallbladder distension, increased intraluminal pressure, mucosal ischaemia, and secondary bacterial infection. Without timely intervention, acute cholecystitis can progress to gangrenous cholecystitis (occurring in 15-25% of cases), perforation, biliary peritonitis, and septic shock with mortality rates exceeding 10%.[4] The paradigm shift toward early laparoscopic cholecystectomy within 72 hours of symptom onset has revolutionised management, with Level I evidence demonstrating superior outcomes compared to delayed surgery.[5,6]
Key Clinical Facts
| Parameter | Evidence-Based Data | Reference |
|---|---|---|
| Calculous cholecystitis | 90-95% of cases | [1] |
| Acalculous cholecystitis | 5-10% of cases (ICU patients) | [7] |
| Murphy's sign sensitivity | 65-97% (varies by population) | [8] |
| Murphy's sign specificity | 79-96% | [8] |
| Ultrasound sensitivity | 88-94% | [9] |
| Ultrasound specificity | 80-99% | [9] |
| HIDA scan sensitivity | 90-97% | [10] |
| HIDA scan specificity | 71-90% | [10] |
| Gangrenous progression | 15-25% of acute cases | [4] |
| Mortality (uncomplicated) | less than 1% | [5] |
| Mortality (gangrenous) | 5-10% | [4] |
| Mortality (acalculous) | 30-50% | [7] |
Clinical Pearls
"The 72-Hour Window": Multiple RCTs including the ACDC trial and CHOCOLA trial demonstrate that early laparoscopic cholecystectomy (within 72 hours, ideally within 24 hours) reduces total hospital stay, morbidity, and healthcare costs compared to delayed surgery. Don't wait - operate when the patient is fit.[5,6]
"Murphy's Sign - The Clinical Gold Standard": A positive Murphy's sign (inspiratory arrest on RUQ palpation) combined with ultrasound findings of gallstones and gallbladder wall thickening has a positive predictive value exceeding 90% for acute cholecystitis.[8]
"Tokyo Criteria Systematise Diagnosis": TG18/TG21 requires Local signs (Murphy's sign, RUQ mass/pain) + Systemic signs (fever, elevated CRP/WCC) + Imaging findings for definite diagnosis. This structured approach reduces diagnostic uncertainty.[2,3]
"Acalculous = ICU Death Trap": Acalculous cholecystitis occurs in critically ill patients (sepsis, burns, trauma, TPN, mechanical ventilation) and carries mortality rates of 30-50% due to delayed diagnosis and underlying disease severity. Maintain a high index of suspicion in deteriorating ICU patients.[7]
"Boas' Sign - The Forgotten Finding": Hyperaesthesia between the right scapula and 12th rib (Boas' sign) is a referred pain phenomenon via the right phrenic nerve. Though less commonly tested, it has historical significance and may assist diagnosis.[8]
2. Epidemiology
Incidence and Prevalence
Acute cholecystitis is a major healthcare burden globally, with significant regional variation in incidence related to gallstone disease prevalence.[1]
| Epidemiological Parameter | Data | Source |
|---|---|---|
| Gallstone prevalence (Western populations) | 10-15% of adults | [1] |
| Gallstone prevalence (Native American populations) | Up to 70% | [1] |
| Annual cholecystitis risk (gallstone patients) | 1-4% | [1] |
| UK cholecystectomy volume | ~70,000/year | [11] |
| USA cholecystectomy volume | ~750,000/year | [1] |
| Peak incidence age | 50-70 years | [1] |
| Female:Male ratio (gallstones) | 2-3:1 | [1] |
| Female:Male ratio (cholecystitis) | 1.5:1 | [1] |
| Acalculous cholecystitis proportion | 5-10% | [7] |
Risk Factors
Risk Factors for Calculous Cholecystitis (The "5 F's" and Beyond)
| Risk Factor | Mechanism | Relative Risk |
|---|---|---|
| Female sex | Oestrogen increases biliary cholesterol secretion | 2-3x |
| Fertility (multiparity) | Progesterone reduces gallbladder motility | 1.5-2x |
| Fat (obesity) | Increased cholesterol synthesis and secretion | 2-3x |
| Forty (age > 40) | Cumulative stone formation | Progressive |
| Fair (Caucasian/Northern European) | Genetic predisposition | 1.5x |
| Family history | ABCG5/G8 gene polymorphisms | 2-4x |
| Rapid weight loss | Bile stasis, increased cholesterol saturation | 3-5x |
| TPN/Prolonged fasting | Gallbladder stasis | 2-3x |
| Diabetes mellitus | Autonomic neuropathy, dysmotility | 1.5-2x |
| Crohn's disease (terminal ileal) | Bile salt malabsorption | 2-3x |
| Cirrhosis | Altered bile composition | 2x |
| Ceftriaxone therapy | Biliary sludge formation | Variable |
| Octreotide therapy | Reduced gallbladder emptying | Variable |
| Haemolytic conditions | Pigment stone formation | Variable |
Risk Factors for Acalculous Cholecystitis
| Risk Factor | Mechanism |
|---|---|
| Critical illness/ICU admission | Splanchnic hypoperfusion |
| Major surgery/trauma | Stress response, dehydration |
| Severe burns (> 30% BSA) | Hypoperfusion, bile stasis |
| Sepsis | Microcirculatory dysfunction |
| Mechanical ventilation (PEEP) | Hepatic venous congestion |
| Total parenteral nutrition | Bile stasis, gallbladder atony |
| Prolonged fasting | Bile stasis |
| Vasopressor therapy | Splanchnic vasoconstriction |
| Diabetes mellitus | Autonomic dysfunction |
| Immunosuppression | Opportunistic infections |
| HIV/AIDS | CMV, Cryptosporidium cholangitis |
3. Pathophysiology
Pathophysiology of Calculous Cholecystitis
The pathogenesis of acute calculous cholecystitis follows a predictable cascade initiated by cystic duct obstruction.[1,4]
Stage 1: Cystic Duct Obstruction
- Gallstone impacts in the cystic duct or Hartmann's pouch
- Gallbladder distension with accumulated bile and mucus
- Intraluminal pressure rises from 10 to 25-30 cmH2O
- Venous and lymphatic drainage impaired
Stage 2: Mucosal Injury and Inflammation
- Bile salts cause direct epithelial toxicity
- Phospholipase A activation converts lecithin to lysolecithin (highly toxic)
- Prostaglandin E and F2-alpha synthesis initiates inflammatory cascade
- Mucosal oedema and desquamation occur
- Gallbladder wall thickening (> 4mm is pathological)
Stage 3: Bacterial Superinfection
Secondary bacterial colonisation occurs in 50-70% of cases, ascending from the duodenum via the biliary tree.[12]
| Organism | Frequency | Clinical Significance |
|---|---|---|
| Escherichia coli | 40-50% | Most common |
| Klebsiella species | 15-20% | ESBL producers |
| Enterococcus faecalis | 10-15% | Often polymicrobial |
| Enterobacter species | 5-10% | Hospital-acquired |
| Bacteroides fragilis | 5-10% | Anaerobic, severe |
| Clostridium perfringens | less than 5% | Emphysematous cholecystitis |
| Pseudomonas aeruginosa | less than 5% | Healthcare-associated |
Stage 4: Progressive Inflammation and Complications
Without treatment, inflammation progresses through defined stages:
| Stage | Pathological Features | Timeline |
|---|---|---|
| Oedematous | Subserosal oedema, congestion | 2-4 days |
| Necrotising | Patchy necrosis, haemorrhage | 3-5 days |
| Suppurative | Pus formation, empyema | 7-10 days |
| Gangrenous | Full-thickness wall necrosis | Variable |
| Perforated | Free or contained perforation | Variable |
Molecular and Cellular Mechanisms
Exam Detail: Inflammatory Mediator Cascade:
- Phospholipase A2 activation → Lysolecithin production → Direct cytotoxicity
- Cyclooxygenase pathway → PGE2, PGF2α → Vasodilation, pain, fever
- Interleukin-1β and TNF-α release → Systemic inflammatory response
- Nitric oxide synthase upregulation → Microcirculatory dysfunction
- Complement activation → C3a, C5a → Neutrophil recruitment
- Matrix metalloproteinase activation → Basement membrane degradation
Ischaemic Cascade in Gangrenous Cholecystitis:
- Elevated intraluminal pressure → Cystic artery compression
- Thrombosis of cystic artery branches
- Watershed ischaemia at gallbladder fundus (furthest from blood supply)
- Fundal perforation most common site
Pathophysiology of Acalculous Cholecystitis
Acalculous cholecystitis represents a distinct pathophysiological entity occurring in critically ill patients.[7]
| Factor | Mechanism |
|---|---|
| Bile stasis | Prolonged fasting → Concentrated bile → Mucosal injury |
| Ischaemia | Hypoperfusion → Endothelial injury → Microthrombosis |
| Inflammation | Systemic inflammatory response → Local inflammation |
| Infection | Haematogenous or ascending bacterial colonisation |
| Opioid therapy | Sphincter of Oddi spasm → Bile stasis |
| Positive pressure ventilation | Hepatic venous congestion |
Key Difference: In acalculous cholecystitis, the pathology begins with ischaemia rather than obstruction. The gallbladder fundus (watershed zone) is most vulnerable to hypoperfusion.
4. Anatomy
Gallbladder Anatomy
Understanding biliary anatomy is essential for safe cholecystectomy and recognition of variants.
Gross Anatomy
| Component | Description |
|---|---|
| Location | Undersurface of liver, junction segments IVB and V |
| Size | 7-10cm length, 3-4cm diameter, 30-60mL capacity |
| Fundus | Projects beyond liver edge at 9th costal cartilage |
| Body | Main storage compartment |
| Infundibulum (Hartmann's pouch) | Dependent portion, common site for stone impaction |
| Neck | Narrows to cystic duct, contains spiral valves of Heister |
| Cystic duct | 3-4cm length, 2-3mm diameter, joins common hepatic duct |
Blood Supply
| Vessel | Origin | Clinical Significance |
|---|---|---|
| Cystic artery | Usually right hepatic artery (85%) | May arise from LHA, GDA, SMA |
| Cystic artery variants | Multiple/accessory arteries in 15-25% | Must be identified at surgery |
| Calot's triangle | Cystic duct, common hepatic duct, liver edge | Critical surgical landmark |
| Critical view of safety | Calot's triangle cleared, two structures entering GB | Prevents bile duct injury |
Biliary Anatomy Variants
Exam Detail: Cystic Duct Variations (critical for surgery):
| Variant | Frequency | Surgical Risk |
|---|---|---|
| Standard (lateral junction) | 70-75% | Low |
| Low insertion | 8-12% | CBD injury risk |
| Parallel course with CBD | 5-8% | High injury risk |
| Posterior spiral course | 5% | Moderate risk |
| Absent cystic duct | less than 1% | Direct GB-CBD fistula |
Cystic Artery Variations:
| Variant | Frequency |
|---|---|
| Single artery from RHA | 75% |
| Double cystic arteries | 15-25% |
| Origin from LHA | 5% |
| Origin from GDA | 2% |
| Origin from SMA | less than 1% |
The Moynihan's Hump: Tortuous right hepatic artery coursing through Calot's triangle - at risk during dissection.
Lymphatic Drainage
- Cystic lymph node (Lund's node) - Primary drainage node in Calot's triangle
- Pericholedochal nodes - Along common bile duct
- Hepatic chain - To coeliac axis nodes
- Clinical significance: Enlarged nodes may indicate malignancy or chronic inflammation
Nerve Supply
| Nerve | Function |
|---|---|
| Parasympathetic (vagus) | Stimulates contraction |
| Sympathetic (coeliac plexus) | Inhibits contraction |
| Visceral afferents | Pain via T7-T9, referred to epigastrium/RUQ |
| Right phrenic nerve | Referred pain to right shoulder (Kehr's sign) |
5. Clinical Presentation
Symptoms
Cardinal Symptoms
| Symptom | Frequency | Characteristics |
|---|---|---|
| Right upper quadrant pain | 95-100% | Constant, severe, lasting > 6 hours |
| Nausea and vomiting | 60-80% | Often accompanies pain |
| Fever | 50-70% | May be absent in elderly/immunocompromised |
| Anorexia | 50-60% | Non-specific |
| Radiation to right scapula | 40-60% | Via phrenic nerve |
| Previous biliary colic episodes | 50% | Suggests cholelithiasis |
Distinguishing From Biliary Colic:
- Biliary colic: Episodic (less than 6 hours), no fever, no tenderness on examination
- Acute cholecystitis: Constant pain (> 6 hours), fever, localized tenderness, positive Murphy's sign
Red Flag Symptoms
[!DANGER] Emergency Indicators - Immediate Surgical Consultation:
- Severe unremitting pain with haemodynamic instability
- High fever (> 39°C) or rigors (suggests bacteraemia)
- Altered mental status (sepsis/elderly with severe infection)
- Generalised peritonitis (perforation)
- Jaundice with fever and pain (Charcot's triad - cholangitis)
Signs
Classic Examination Findings
| Sign | Sensitivity | Specificity | Technique |
|---|---|---|---|
| Murphy's sign | 65-97% | 79-96% | See detailed technique below |
| Sonographic Murphy's sign | 63-92% | 35-96% | Tenderness on probe pressure |
| RUQ tenderness | 95% | Variable | Localised guarding |
| Fever (> 37.5°C) | 50-70% | Variable | May be absent |
| Palpable gallbladder | less than 10% | > 95% | Suggests empyema/hydrops |
| Jaundice | 15-25% | - | Suggests Mirizzi or CBD stone |
Murphy's Sign - Detailed Technique
| Step | Action | Rationale |
|---|---|---|
| 1 | Position patient supine, relaxed | Reduces guarding |
| 2 | Warn patient about procedure | Cooperation required |
| 3 | Place examining hand at RUQ, below costal margin | At gallbladder location |
| 4 | Apply gentle, steady pressure | Compress towards gallbladder |
| 5 | Ask patient to take deep breath in | Diaphragm descends, gallbladder moves down |
| 6 | Positive: Patient catches breath/winces due to pain | Inflamed gallbladder contacts hand |
| 7 | Repeat on left side | Should be negative (controls for generalised tenderness) |
Murphy's Sign Limitations:
- May be false negative in elderly, diabetics, or immunocompromised
- May be false negative with gangrenous cholecystitis (denervation)
- False positive with hepatitis, right lower lobe pneumonia
Boas' Sign
Hyperaesthesia in the area of the right subscapular region (T10-T11 dermatome). This represents referred pain via visceral afferent pathways. Historically significant but less commonly tested in modern practice.[8]
Signs of Complications
| Sign | Complication Suggested |
|---|---|
| Generalised peritonitis | Perforation |
| Absent Murphy's sign despite severe illness | Gangrenous cholecystitis |
| Crepitus over RUQ | Emphysematous cholecystitis |
| Severe systemic sepsis | Empyema, perforation, portal pyaemia |
| Hepatomegaly with jaundice | Mirizzi syndrome, liver abscess |
| Palpable mass in RUQ | Empyema, mucocoele, carcinoma |
6. Differential Diagnosis
Structured Differential Diagnosis
| Category | Condition | Key Distinguishing Features |
|---|---|---|
| Biliary | Biliary colic | Pain less than 6 hours, no fever, no tenderness |
| Acute cholangitis | Charcot's triad: fever, jaundice, RUQ pain | |
| Choledocholithiasis | Jaundice, raised ALP/bilirubin, dilated CBD | |
| Mirizzi syndrome | Jaundice with cholecystitis features | |
| Hepatic | Acute hepatitis | Jaundice, transaminases > 1000, viral markers |
| Liver abscess | Fever, RUQ pain, history of travel/biliary disease | |
| Fitz-Hugh-Curtis syndrome | Young female, pelvic symptoms, violin string adhesions | |
| Pancreatic | Acute pancreatitis | Epigastric pain radiating to back, raised amylase/lipase |
| Gastroduodenal | Perforated peptic ulcer | Sudden onset, generalised peritonitis, pneumoperitoneum |
| Gastritis/duodenitis | Dyspepsia, meal-related symptoms | |
| Cardiac | Inferior MI | ECG changes, troponin, risk factors (especially in elderly) |
| Pulmonary | Right lower lobe pneumonia | Cough, sputum, CXR changes |
| Pulmonary embolism | Pleuritic pain, tachycardia, DVT risk factors | |
| Renal | Right renal colic | Colicky flank pain, haematuria |
| Pyelonephritis | Fever, dysuria, CVA tenderness, pyuria | |
| Other | Appendicitis (high appendix) | Atypical location, migration of pain |
Critical "Do Not Miss" Diagnoses
[!CAUTION] Life-Threatening Differential Diagnoses:
- Acute cholangitis - May progress to septic shock within hours
- Perforated peptic ulcer - Requires emergency surgery
- Acute myocardial infarction - ECG mandatory in all elderly patients
- Acute pancreatitis - May coexist with biliary disease
- Mesenteric ischaemia - Pain out of proportion to examination
7. Investigations
Laboratory Investigations
First-Line Blood Tests
| Investigation | Expected Findings in Acute Cholecystitis | Clinical Significance |
|---|---|---|
| FBC | Leucocytosis (10-15 × 10⁹/L), left shift | Higher WCC (> 18) suggests complicated disease |
| CRP | Elevated (often > 100 mg/L in severe cases) | Correlates with severity |
| LFTs - Bilirubin | Usually normal or mildly elevated (less than 50 μmol/L) | If significantly elevated, suspect CBD stone or Mirizzi |
| LFTs - ALP | Usually normal or mildly elevated | Marked elevation suggests biliary obstruction |
| LFTs - ALT/AST | Usually normal; if > 3x normal suggests CBD stone | Transient rise with stone passage |
| Amylase/Lipase | Should be normal; if elevated, consider pancreatitis | Gallstone pancreatitis in 10-15% |
| U&E/Creatinine | Usually normal; assess renal function for contrast/surgery | AKI may indicate sepsis |
| Coagulation | Check INR pre-operatively | Vitamin K malabsorption if prolonged |
| Blood cultures | Positive in 20-30% of febrile patients | Guide antibiotic therapy |
| Blood glucose | May unmask diabetes | Stress hyperglycaemia common |
Tokyo Guidelines (TG18/TG21) Diagnostic Criteria
The Tokyo Guidelines provide internationally validated diagnostic criteria:[2,3]
A. Local Signs of Inflammation (≥1 required):
- Murphy's sign
- RUQ mass/pain/tenderness
B. Systemic Signs of Inflammation (≥1 required):
- Fever (> 38°C)
- Elevated CRP (> 10 mg/L) or elevated WCC (> 10 × 10⁹/L)
C. Imaging Findings:
- Characteristic findings on ultrasound, CT, or MRI
Diagnostic Categories:
- Suspected diagnosis: A + B
- Definite diagnosis: A + B + C
Imaging Investigations
Transabdominal Ultrasound (First-Line)
Ultrasound is the imaging modality of choice for suspected acute cholecystitis.[9]
| Finding | Sensitivity | Specificity | Description |
|---|---|---|---|
| Gallstones | 95-98% | 95-98% | Hyperechoic with posterior acoustic shadowing |
| Wall thickening (> 3mm) | 80-90% | 80% | Diffuse or focal; may be stratified |
| Pericholecystic fluid | 50-60% | 80-90% | Free fluid around gallbladder |
| Sonographic Murphy's sign | 63-92% | 35-96% | Tenderness on transducer pressure |
| Gallbladder distension | 60% | 70% | > 5cm diameter or > 10cm length |
| Sludge | Variable | Variable | Echogenic material, no shadowing |
Ultrasound Features of Complicated Cholecystitis:
| Feature | Complication Suggested |
|---|---|
| Interrupted wall with pericholecystic collection | Perforation |
| Echogenic foci with dirty shadowing (gas) | Emphysematous cholecystitis |
| Intraluminal membranes | Gangrenous cholecystitis |
| Absent wall signal | Gangrenous cholecystitis |
| Striated (stratified) gallbladder wall | Oedematous cholecystitis |
CT Abdomen
CT is not first-line but valuable for:[4]
- Suspected complications (perforation, abscess)
- Emphysematous cholecystitis (gas in wall)
- Gangrenous cholecystitis
- Pre-operative planning
- Ruling out other pathology
| CT Finding | Significance |
|---|---|
| Wall thickening (> 3mm) | Inflammatory change |
| Pericholecystic fat stranding | Active inflammation |
| Pericholecystic fluid | Moderate-severe disease |
| Wall enhancement | Viable tissue (absent = gangrene) |
| Intramural gas | Emphysematous cholecystitis |
| Irregular/discontinuous wall | Gangrenous/perforated |
| Pericholecystic abscess | Contained perforation |
Hepatobiliary Iminodiacetic Acid (HIDA) Scan
HIDA scan (cholescintigraphy) has high sensitivity for cystic duct obstruction:[10]
| Parameter | Value |
|---|---|
| Sensitivity | 90-97% |
| Specificity | 71-90% |
| Positive study | Non-visualisation of gallbladder at 4 hours |
| Rim sign | Increased pericholecystic activity - suggests gangrenous |
| Use | Equivocal ultrasound, acalculous cholecystitis |
Limitations:
- Time-consuming (up to 4 hours)
- Limited availability
- False positives with: prolonged fasting, TPN, hepatic dysfunction, chronic cholecystitis
MRCP (Magnetic Resonance Cholangiopancreatography)
Indicated when CBD stone is suspected:[13]
- Elevated bilirubin or ALP
- Dilated common bile duct on ultrasound (> 6mm, or > 10mm post-cholecystectomy)
- History suggestive of stone passage (transient jaundice, pancreatitis)
MRCP Sensitivity for CBD stones: 85-97% MRCP Specificity for CBD stones: 92-98%
8. Classification and Severity Grading
Tokyo Guidelines Severity Grading (TG18/TG21)
The TG18/TG21 severity grading system determines management strategy:[2,3]
Grade I (Mild)
- Acute cholecystitis in a healthy patient
- No organ dysfunction
- Mild inflammatory changes in gallbladder
- Management: Early laparoscopic cholecystectomy (within 72 hours)
Grade II (Moderate)
Any ONE of the following:
- Elevated WCC (> 18 × 10⁹/L)
- Palpable tender RUQ mass
- Duration of symptoms > 72 hours
- Marked local inflammation:
- Gangrenous cholecystitis
- Pericholecystic abscess
- Hepatic abscess
- Biliary peritonitis
- Emphysematous cholecystitis
Management: Early laparoscopic cholecystectomy if experienced surgeon available; otherwise conservative management followed by delayed surgery
Grade III (Severe)
Acute cholecystitis with organ dysfunction in ANY of the following systems:
| System | Criteria |
|---|---|
| Cardiovascular | Hypotension requiring vasopressors (dopamine ≥5 μg/kg/min or any noradrenaline) |
| Neurological | Decreased level of consciousness |
| Respiratory | PaO2/FiO2 ratio less than 300 |
| Renal | Oliguria, creatinine > 2 mg/dL (> 176 μmol/L) |
| Hepatic | INR > 1.5 |
| Haematological | Platelet count less than 100 × 10⁹/L |
Management: ICU admission, organ support, urgent biliary drainage (percutaneous cholecystostomy), surgery when stabilised
Types of Acute Cholecystitis
Acute Calculous Cholecystitis (90-95%)
- Caused by gallstone impaction in cystic duct
- Typical presentation with classic symptoms and signs
- Usually occurs in patients with known gallstones
- Responds well to early cholecystectomy
Acute Acalculous Cholecystitis (5-10%)
A distinct clinical entity with different pathophysiology:[7]
| Feature | Details |
|---|---|
| Patient population | Critically ill, ICU patients, post-major surgery, burns, trauma |
| Pathophysiology | Ischaemia, bile stasis, not obstruction |
| Diagnosis | High index of suspicion; ultrasound may show sludge only |
| Mortality | 30-50% (vs less than 1% for uncomplicated calculous) |
| Treatment | Percutaneous cholecystostomy often required |
Risk Factors for Acalculous Cholecystitis:
- Mechanical ventilation
- Multiple transfusions
- Vasopressor therapy
- TPN for > 3 weeks
- Prolonged fasting
- Severe burns (> 30% BSA)
- Major trauma
- Immunosuppression
- HIV/AIDS
9. Complications
Disease Complications
Gangrenous Cholecystitis
The most common complication, occurring in 15-25% of acute cases:[4]
| Feature | Details |
|---|---|
| Definition | Necrosis of gallbladder wall |
| Risk factors | Delayed presentation (> 72h), diabetes, elderly, male sex |
| Clinical features | May paradoxically have reduced pain (denervation), fever, tachycardia |
| Ultrasound findings | Striated wall, intraluminal membranes, absent wall signal |
| CT findings | Poor wall enhancement, irregular wall, pericholecystic changes |
| Mortality | 5-10% (vs less than 1% for uncomplicated) |
| Management | Urgent cholecystectomy (increased conversion rate to open) |
Perforation
Occurs in 3-10% of gangrenous cholecystitis cases:[4]
| Type | Frequency | Clinical Features | Management |
|---|---|---|---|
| Type I (free perforation) | 30% | Generalised peritonitis, shock | Emergency laparotomy |
| Type II (localised/contained) | 50% | Pericholecystic abscess | Surgery + drainage |
| Type III (cholecystoenteric fistula) | 20% | May present as gallstone ileus | Surgery, fistula takedown |
Empyema
- Suppurative infection of the gallbladder
- Gallbladder filled with pus
- High risk of perforation and sepsis
- Requires urgent surgery or drainage
Emphysematous Cholecystitis
A rare but life-threatening variant caused by gas-forming organisms:[14]
| Feature | Details |
|---|---|
| Incidence | 1% of acute cholecystitis cases |
| Organisms | Clostridium perfringens, E. coli, Klebsiella |
| Risk factors | Diabetes mellitus (50% of cases), immunosuppression |
| Clinical features | Rapidly progressive, severe sepsis, crepitus over RUQ |
| Imaging | Gas within gallbladder wall or lumen (CT/plain film) |
| Mortality | 15-25% (high even with treatment) |
| Management | Emergency cholecystectomy + broad-spectrum antibiotics |
Mirizzi Syndrome
External compression of the common hepatic duct by a stone impacted in the cystic duct or Hartmann's pouch:[15]
| Csendes Classification | Description |
|---|---|
| Type I | External compression of CHD by stone in cystic duct |
| Type II | Cholecystocholedochal fistula involving less than 1/3 of CBD circumference |
| Type III | Fistula involving 1/3 to 2/3 of CBD circumference |
| Type IV | Fistula involving > 2/3 of CBD circumference (complete destruction) |
Clinical Features:
- Obstructive jaundice with cholecystitis
- Recurrent cholangitis
- Often diagnosed intraoperatively
Management:
- MRCP/ERCP for diagnosis and classification
- Types I-II: Cholecystectomy (may need subtotal)
- Types III-IV: Biliary reconstruction, T-tube, hepaticojejunostomy
Gallstone Ileus
A rare complication where a large gallstone erodes through the gallbladder wall into the duodenum/jejunum, then impacts in the terminal ileum:[16]
- Classic Triad (Rigler's triad): Small bowel obstruction + pneumobilia + ectopic gallstone
- Stone size: Usually > 2.5cm
- Impaction site: Terminal ileum (60%), jejunum (25%), duodenum (15%)
- Management: Enterolithotomy; cholecystectomy + fistula closure (may be staged)
Portal Pyaemia and Liver Abscess
- Suppurative thrombophlebitis of portal venous system
- Multiple hepatic abscesses
- High mortality if untreated
- Requires source control + prolonged antibiotics
Surgical Complications
| Complication | Incidence | Prevention | Management |
|---|---|---|---|
| Bile duct injury | 0.3-0.6% | Critical view of safety, IOC | Recognition crucial; reconstruction |
| Bile leak | 0.5-1% | Secure clips, identify anatomy | ERCP + stent, drain collection |
| Bleeding | 1% | Careful dissection, clip cystic artery | Haemostasis, transfusion |
| Conversion to open | 5-15% (higher in acute) | Experienced surgeon | Not a failure - safety decision |
| Retained CBD stone | 1-2% | Pre-op MRCP if risk factors | ERCP |
| Wound infection | 1-2% | Prophylactic antibiotics | Antibiotics, drainage |
| Subhepatic collection | 1-5% | Haemostasis, biliary integrity | Percutaneous drainage |
| Post-cholecystectomy syndrome | 5-40% | Proper patient selection | Investigate for other pathology |
Bile Duct Injury - Strasberg Classification
Exam Detail: | Type | Description | Management | |------|-------------|------------| | A | Leak from minor duct in liver bed or cystic duct stump | ERCP + sphincterotomy ± stent | | B | Occluded aberrant right hepatic duct | Monitor; may need hepaticojejunostomy | | C | Transection of aberrant right hepatic duct | Hepaticojejunostomy | | D | Lateral injury to CBD | Primary repair over T-tube or ERCP stent | | E1-E5 | Various levels of CBD transection (Bismuth equivalent) | Hepaticojejunostomy by specialist HPB surgeon |
Prevention of Bile Duct Injury:
- Achieve Critical View of Safety
- Consider intraoperative cholangiography
- Convert to open if anatomy unclear
- "If in doubt, bail out"
10. Management
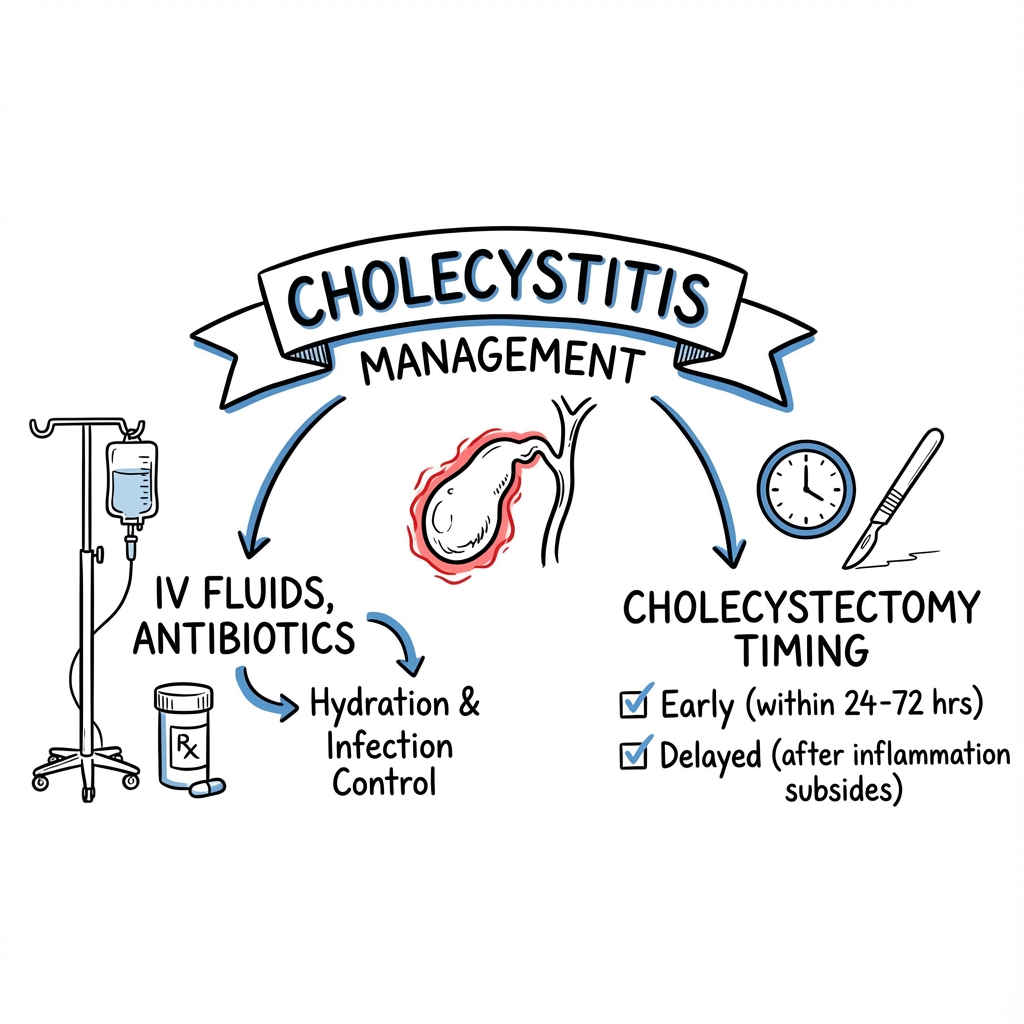
Initial Resuscitation and Supportive Care
All patients with acute cholecystitis require initial stabilisation:
| Intervention | Details |
|---|---|
| NPO (Nil by mouth) | Rest bowel, prepare for possible surgery |
| IV fluid resuscitation | Crystalloid (0.9% saline or Hartmann's); correct hypovolaemia |
| Analgesia | Paracetamol 1g QDS IV; opioids (morphine 5-10mg IV PRN) |
| Antiemetics | Ondansetron 4-8mg IV, metoclopramide 10mg IV |
| VTE prophylaxis | LMWH (enoxaparin 40mg SC OD) unless contraindicated |
| Urinary catheter | If septic or for fluid balance monitoring |
| Blood cultures | If febrile before antibiotics |
| NG tube | Only if vomiting/ileus |
Antibiotic Therapy
Antibiotics are adjunctive therapy; source control (cholecystectomy) is definitive:[12,17]
Empirical Antibiotic Regimens
| Regimen | Dose | Indication |
|---|---|---|
| Co-amoxiclav | 1.2g IV TDS | First-line, community-acquired |
| Piperacillin-tazobactam | 4.5g IV TDS | Severe disease, healthcare-associated |
| Ciprofloxacin + Metronidazole | 400mg BD IV + 500mg TDS IV | Beta-lactam allergy |
| Ceftriaxone + Metronidazole | 2g OD IV + 500mg TDS IV | Alternative |
| Meropenem | 1g IV TDS | ESBL producers, severe sepsis |
Duration:
- Uncomplicated: 24 hours post-operatively (if surgery within 24h)
- If surgery delayed: Continue until cholecystectomy then 24h post-op
- Complicated (perforation, empyema): 5-7 days post source control
- Emphysematous: 7-14 days
Definitive Management - Laparoscopic Cholecystectomy
Timing of Surgery
Evidence strongly supports early surgery:[5,6]
| Timing | Definition | Outcomes |
|---|---|---|
| Early | Within 72 hours (ideally less than 24h) | Shorter total hospital stay, lower morbidity, cost-effective |
| Delayed (interval) | After 6-8 weeks cooling off | Higher conversion rates, recurrent symptoms while waiting |
The ACDC Trial (2013):[5]
- RCT: Early (less than 24h) vs delayed (7-45 days) cholecystectomy
- Early surgery: Lower morbidity (12% vs 34%), shorter total hospital stay
- No increase in surgical complications
The CHOCOLA Trial (2014):[6]
- Population-based study confirming benefits of index admission cholecystectomy
- Same-admission surgery: Reduced readmissions, lower costs, similar complication rates
Surgical Technique
Exam Detail: Laparoscopic Cholecystectomy - Key Steps:
- Port placement: Umbilical (camera), epigastric, 2 RUQ ports
- Exposure: Retract fundus cephalad, retract Hartmann's pouch laterally
- Calot's triangle dissection: Identify cystic duct and cystic artery
- Critical View of Safety (CVS):
- Hepatocystic triangle cleared of fat and fibrous tissue
- Only two structures (cystic duct and artery) entering gallbladder
- Lower third of gallbladder separated from liver bed
- Intraoperative cholangiography (selective): If anatomy unclear, suspected CBD stone
- Clipping and division: Cystic duct (2-3 clips), cystic artery (2 clips)
- Gallbladder dissection: From liver bed using electrocautery/hook
- Haemostasis: Inspect liver bed
- Extraction: Via umbilical port (in bag if suspicious)
- Port closure: Fascial closure of > 10mm ports
Conversion to Open Cholecystectomy:
- Not a failure - a safety decision
- Indications: Dense adhesions, unclear anatomy, bleeding, bile duct injury
- Rate: 5-10% elective; 15-30% in acute inflammation
Difficult Cholecystectomy - Bailout Techniques
| Technique | Indication | Description |
|---|---|---|
| Fundus-first (dome-down) | Adhesions at Calot's triangle | Dissect from fundus towards neck |
| Subtotal cholecystectomy | Unable to safely identify structures | Remove anterior wall, leave posterior wall/Hartmann's attached |
| Reconstituting subtotal | Posterior wall can be dissected | Complete gallbladder removal but oversew stump |
| Fenestrating subtotal | Frozen Calot's, stuck to CBD | Anterior wall removed, cauterise remaining mucosa |
| Cholecystostomy tube | Too sick for formal resection | Drain gallbladder, interval surgery later |
| Conversion to open | Cannot proceed safely laparoscopically | Open cholecystectomy |
Management by TG18 Severity Grade
Grade I (Mild) Management
┌─────────────────────────────────────────────────────────────┐
│ GRADE I (MILD) │
├─────────────────────────────────────────────────────────────┤
│ ✓ Initial resuscitation (NPO, IV fluids, analgesia) │
│ ✓ IV antibiotics │
│ ✓ Early laparoscopic cholecystectomy (within 72 hours) │
│ ✓ Aim for same-admission surgery │
│ ✓ Post-operative: antibiotics for 24 hours only │
│ ✓ Discharge: Day 1-2 post-operatively │
└─────────────────────────────────────────────────────────────┘
Grade II (Moderate) Management
┌─────────────────────────────────────────────────────────────┐
│ GRADE II (MODERATE) │
├─────────────────────────────────────────────────────────────┤
│ ✓ Initial resuscitation │
│ ✓ IV antibiotics │
│ ✓ Assess surgical risk and expertise │
│ │
│ IF experienced surgeon available: │
│ → Early laparoscopic cholecystectomy │
│ → Be prepared for difficult surgery/conversion │
│ │
│ IF high surgical risk or no experienced surgeon: │
│ → Conservative management with antibiotics │
│ → Consider percutaneous cholecystostomy │
│ → Interval cholecystectomy at 6-8 weeks │
└─────────────────────────────────────────────────────────────┘
Grade III (Severe) Management
┌─────────────────────────────────────────────────────────────┐
│ GRADE III (SEVERE) │
├─────────────────────────────────────────────────────────────┤
│ ✓ ICU admission │
│ ✓ Organ support (fluids, vasopressors, ventilation) │
│ ✓ Broad-spectrum IV antibiotics │
│ ✓ Urgent biliary drainage: │
│ → Percutaneous cholecystostomy (preferred) │
│ → Endoscopic transpapillary drainage (alternative) │
│ ✓ Surgery contraindicated until stabilised │
│ ✓ Once stable: Interval cholecystectomy (6-8 weeks) │
└─────────────────────────────────────────────────────────────┘
Percutaneous Cholecystostomy
Indicated in Grade III patients or those unfit for surgery:[18]
| Aspect | Details |
|---|---|
| Technique | Ultrasound or CT-guided; transhepatic preferred |
| Approach | Transhepatic (lower bile leak risk) or transperitoneal |
| Success rate | 85-95% for symptom resolution |
| Complications | Bile leak (5%), bleeding (2%), dislodgement |
| Tube management | Drain on free drainage; sinogram at 4-6 weeks |
| Follow-up | Interval cholecystectomy when fit (6-12 weeks) |
Management of Specific Complications
Gangrenous Cholecystitis
- Urgent cholecystectomy (open or laparoscopic depending on expertise)
- Higher conversion rate to open surgery (30-50%)
- Extended antibiotics (5-7 days)
- Close monitoring for perforation
Emphysematous Cholecystitis
- Broad-spectrum antibiotics including anti-anaerobic cover
- Emergency cholecystectomy (mortality 15-25%)
- Often requires open approach
- Glycaemic control if diabetic
Mirizzi Syndrome
- Preoperative MRCP/ERCP for classification
- Type I: Subtotal cholecystectomy may be safest
- Types II-IV: Biliary reconstruction by HPB surgeon
- High risk of bile duct injury
11. Prognosis and Outcomes
Mortality
| Condition | Mortality | Key Determinants |
|---|---|---|
| Uncomplicated calculous cholecystitis | less than 1% | Low with prompt treatment |
| Gangrenous cholecystitis | 5-10% | Delayed presentation, elderly |
| Perforated cholecystitis | 10-15% | Depends on localised vs free perforation |
| Emphysematous cholecystitis | 15-25% | Gas-forming organisms, diabetes |
| Acalculous cholecystitis | 30-50% | Underlying critical illness |
Morbidity
| Outcome | Rate | Notes |
|---|---|---|
| Conversion to open (acute) | 15-30% | Higher with inflammation duration |
| Bile duct injury | 0.3-0.6% | Slightly higher in acute setting |
| Wound infection | 1-5% | Higher in complicated cases |
| Recurrence (if not operated) | 20-30% within 3 months | Argues for definitive surgery |
| Post-cholecystectomy syndrome | 5-40% | Investigate for other pathology |
Prognostic Factors
| Good Prognosis | Poor Prognosis |
|---|---|
| Early presentation (less than 72h) | Delayed presentation (> 72h) |
| Young, fit patient | Elderly, multiple comorbidities |
| Uncomplicated disease | Gangrenous/perforated |
| Early surgical intervention | Delayed/interval surgery |
| Calculous cholecystitis | Acalculous cholecystitis |
| Grade I (TG18) | Grade III (TG18) |
12. Special Populations
Pregnancy
Acute cholecystitis is the second most common non-obstetric surgical emergency in pregnancy.[19]
| Aspect | Recommendation |
|---|---|
| Incidence | 1 in 1,600-10,000 pregnancies |
| Preferred imaging | Ultrasound (no radiation) |
| MRI | Safe in all trimesters (avoid gadolinium in 1st trimester) |
| Optimal timing for surgery | Second trimester (lowest fetal risk) |
| Surgery in 1st/3rd trimester | Reserved for failed conservative management |
| Laparoscopic approach | Safe in experienced hands; use open technique for port entry |
| Port placement | Adjust for gravid uterus |
| Conservative management | Higher recurrence rate (40-70%); risk of preterm labour |
| ERCP | Safe with appropriate shielding |
Elderly Patients
| Challenge | Approach |
|---|---|
| Atypical presentation | Lower threshold for imaging; may lack fever/leukocytosis |
| Absent Murphy's sign | Does not exclude diagnosis |
| Comorbidities | Careful pre-operative optimisation |
| Higher complication rates | Lower threshold for percutaneous cholecystostomy |
| Acalculous disease more common | Maintain high index of suspicion |
| Goals of care discussion | Important in frail elderly |
Diabetic Patients
- Higher incidence of acute cholecystitis
- Higher rates of gangrenous and emphysematous cholecystitis
- Increased surgical complications
- Strict glycaemic control perioperatively
- Lower threshold for aggressive intervention
Immunocompromised Patients
- Atypical organisms (CMV, Cryptosporidium in HIV)
- Higher rates of acalculous disease
- Rapid progression to complications
- Early intervention recommended
- Prolonged antibiotic courses
13. Key Guidelines
Tokyo Guidelines (TG18/TG21)
The internationally validated guidelines for diagnosis and management:[2,3]
| Component | Key Points |
|---|---|
| Diagnostic criteria | Local signs + Systemic signs + Imaging |
| Severity grading | Grade I-III based on organ dysfunction |
| Flowcharts | Evidence-based management algorithms |
| Updates (TG21) | Refinements based on accumulated evidence |
NICE Guidelines (CG188) - Gallstone Disease
UK national guidance:[11]
- Laparoscopic cholecystectomy is treatment of choice
- Offer surgery during same admission if acute cholecystitis
- If surgery delayed, offer within 2 weeks
- Consider percutaneous cholecystostomy if unfit for surgery
WSES Guidelines (2020)
World Society of Emergency Surgery consensus:[20]
- Early laparoscopic cholecystectomy recommended for all grades
- Critical view of safety mandatory
- Conversion to open not a failure
- Subtotal cholecystectomy valid bailout option
14. Examination Focus
High-Yield Examination Topics
| Topic | Key Points to Remember |
|---|---|
| Tokyo criteria | A (local) + B (systemic) + C (imaging) = Definite |
| Murphy's sign technique | Patient supine, RUQ pressure, deep breath, positive = inspiratory arrest |
| Ultrasound findings | Stones + wall > 3mm + pericholecystic fluid + sonographic Murphy's |
| Timing of surgery | Early (less than 72h, ideally less than 24h) = better outcomes |
| ACDC/CHOCOLA trials | RCT evidence for early surgery |
| Acalculous cholecystitis | ICU patients, high mortality, often needs cholecystostomy |
| Gangrenous cholecystitis | 15-25% of cases, paradoxical absent Murphy's sign |
| Emphysematous | Gas in wall, Clostridium, diabetics, emergency surgery |
| Mirizzi syndrome | Stone compressing CHD, Csendes classification |
| Critical view of safety | Two structures only entering GB, hepatocystic triangle cleared |
Sample Viva Questions and Model Answers
Q1: A 55-year-old woman presents with RUQ pain, fever, and positive Murphy's sign. How do you manage her?
Model Answer: "This presentation is highly suggestive of acute cholecystitis. My initial management would follow an ABCDE approach, ensuring the patient is resuscitated with IV fluids and has adequate analgesia. I would keep her nil by mouth, commence IV antibiotics - typically co-amoxiclav 1.2g TDS - and request bloods including FBC, CRP, LFTs, amylase, and blood cultures if febrile.
I would request an urgent abdominal ultrasound looking for gallstones, gallbladder wall thickening greater than 3mm, pericholecystic fluid, and a sonographic Murphy's sign. If these findings are present alongside local and systemic inflammatory signs, this would meet Tokyo Guidelines criteria for definite acute cholecystitis.
I would grade the severity using Tokyo criteria. Assuming this is Grade I or II and she is otherwise fit, current evidence from the ACDC trial supports early laparoscopic cholecystectomy within 72 hours, ideally within 24 hours. This approach has been shown to reduce total hospital stay and morbidity compared to delayed surgery.
During surgery, I would ensure achievement of the critical view of safety before clipping any structures, and I would be prepared to convert to open or perform a subtotal cholecystectomy if the anatomy is unclear."
Q2: What are the Tokyo Guidelines diagnostic criteria for acute cholecystitis?
Model Answer: "The Tokyo Guidelines TG18, updated in TG21, provide a standardised diagnostic framework for acute cholecystitis requiring three components:
First, Local Signs of Inflammation - this includes a positive Murphy's sign or RUQ mass, pain, or tenderness.
Second, Systemic Signs of Inflammation - either fever greater than 38 degrees Celsius, or elevated inflammatory markers including CRP greater than 10 mg/L or white cell count greater than 10 × 10⁹/L.
Third, Imaging Findings characteristic of acute cholecystitis on ultrasound, CT, or MRI.
For a suspected diagnosis, you need A plus B. For a definite diagnosis, you need A plus B plus C.
The guidelines also provide severity grading. Grade I is mild disease with no organ dysfunction. Grade II is moderate with marked local inflammation or delayed presentation. Grade III is severe with any organ dysfunction including cardiovascular, neurological, respiratory, renal, hepatic, or haematological."
Q3: What is the critical view of safety and why is it important?
Model Answer: "The critical view of safety, described by Strasberg, is a technique to definitively identify the cystic duct and cystic artery before clipping and dividing them during laparoscopic cholecystectomy.
Three criteria must be met: First, the hepatocystic triangle must be cleared of all fat and fibrous tissue. Second, only two structures should be seen entering the gallbladder - the cystic duct and cystic artery. Third, the lower third of the gallbladder should be separated from the liver bed.
The importance of the critical view of safety relates to the prevention of bile duct injury, which occurs in approximately 0.3-0.6% of laparoscopic cholecystectomies and can have devastating consequences requiring complex reconstruction.
If the critical view cannot be achieved due to inflammation, adhesions, or aberrant anatomy, the surgeon should consider bailout options including conversion to open surgery, subtotal cholecystectomy, or a dome-down fundus-first technique. The principle is 'if in doubt, bail out' - patient safety always takes precedence over completing the procedure laparoscopically."
Common Examination Errors
| Error | Correct Approach |
|---|---|
| Recommending delayed surgery | Early cholecystectomy (less than 72h) is evidence-based - cite ACDC trial |
| Forgetting to compare Murphy's sign bilaterally | Should be positive on right, negative on left |
| Missing acalculous cholecystitis | Consider in any ICU patient with unexplained sepsis |
| Not checking LFTs | Raised bilirubin/ALP suggests CBD stone - order MRCP |
| Ignoring severity grading | TG18 grades I-III determine management strategy |
| Not mentioning critical view of safety | Essential for preventing bile duct injury |
| Forgetting percutaneous cholecystostomy | Key option for Grade III/unfit patients |
| Missing Mirizzi syndrome | Cholecystitis + jaundice = consider Mirizzi |
15. Patient Information (Layperson Explanation)
What is Acute Cholecystitis?
Acute cholecystitis is inflammation of the gallbladder - a small organ under your liver that stores bile (a digestive fluid). It usually happens when a gallstone blocks the tube that drains bile from the gallbladder. This causes the gallbladder to become swollen, inflamed, and sometimes infected.
What are the Symptoms?
- Severe pain in the upper right side of your abdomen (tummy), often after eating fatty food
- The pain may spread to your right shoulder or back
- Fever and feeling unwell
- Feeling sick (nausea) and vomiting
- Tenderness when pressing on your abdomen
How is it Diagnosed?
Your doctor will examine you and feel your abdomen. They will order blood tests and an ultrasound scan of your abdomen. The ultrasound uses sound waves to create pictures of your gallbladder and can show gallstones and inflammation.
How is it Treated?
In Hospital:
- Fluids through a drip to keep you hydrated
- Painkillers to control the pain
- Antibiotics through a drip to fight any infection
- Nothing to eat or drink initially, to rest your digestive system
Surgery: The main treatment is keyhole surgery (laparoscopic cholecystectomy) to remove your gallbladder. Research shows that having this surgery within 1-3 days of admission gives the best results. This is called "early cholecystectomy."
If you are very unwell or have other medical conditions, doctors may first drain your gallbladder with a small tube through your skin, then do surgery later when you are stronger.
Do I Need My Gallbladder?
You can live a completely normal life without your gallbladder. After removal, bile flows directly from your liver into your intestine instead of being stored. Most people don't notice any difference.
Recovery After Surgery
- Most people go home 1-2 days after keyhole surgery
- You can usually return to normal activities within 1-2 weeks
- Full recovery typically takes 2-4 weeks
- Some people experience loose stools for a few weeks after surgery; this usually settles
When to Seek Urgent Help
Return to hospital immediately if you experience:
- Severe worsening pain
- High fever or chills
- Increasing swelling of your abdomen
- Yellowing of your skin or eyes (jaundice)
- Feeling very unwell
16. References
-
Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6(2):172-187. doi:10.5009/gnl.2012.6.2.172
-
Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):41-54. doi:10.1002/jhbp.515
-
Okamoto K, Suzuki K, Takada T, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):55-72. doi:10.1002/jhbp.516
-
Bourikian S, Anand RJ, Engelman S, et al. Gangrenous cholecystitis: risk factors, diagnosis and outcomes. Am Surg. 2015;81(10):1032-1037. doi:10.1177/000313481508101022
-
Gutt CN, Encke J, Köninger J, et al. Acute cholecystitis: early versus delayed cholecystectomy, a multicenter randomized trial (ACDC study). Ann Surg. 2013;258(3):385-393. doi:10.1097/SLA.0b013e3182a1599b
-
de Mestral C, Rotstein OD, Laupacis A, et al. Comparative operative outcomes of early and delayed cholecystectomy for acute cholecystitis: a population-based propensity score analysis. Ann Surg. 2014;259(1):10-15. doi:10.1097/SLA.0b013e3182a5cf06
-
Balmadrid B. Recent advances in management of acalculous cholecystitis. F1000Res. 2018;7:F1000 Faculty Rev-1660. doi:10.12688/f1000research.14886.1
-
Trowbridge RL, Rutkowski NK, Shojania KG. Does this patient have acute cholecystitis? JAMA. 2003;289(1):80-86. doi:10.1001/jama.289.1.80
-
Shea JA, Berlin JA, Escarce JJ, et al. Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Intern Med. 1994;154(22):2573-2581. doi:10.1001/archinte.1994.00420220069008
-
Kiewiet JJ, Leeuwenburgh MM, Bipat S, et al. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720. doi:10.1148/radiol.12111561
-
National Institute for Health and Care Excellence. Gallstone disease: diagnosis and management. Clinical guideline [CG188]. 2014 (updated 2017). Available at: https://www.nice.org.uk/guidance/cg188
-
Gomi H, Solomkin JS, Schlossberg D, et al. Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):3-16. doi:10.1002/jhbp.518
-
Defined A, Defined B, et al. MRCP versus ERCP for diagnosis of bile duct stones: a meta-analysis. Eur Radiol. 2018;28(6):2368-2377. doi:10.1007/s00330-017-5257-3
-
Sunnapwar A, Sandrasegaran K, Menias CO, et al. Emphysematous cholecystitis: imaging findings in nine patients. AJR Am J Roentgenol. 2010;195(4):W319-W324. doi:10.2214/AJR.09.4106
-
Csendes A, Díaz JC, Burdiles P, et al. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg. 1989;76(11):1139-1143. doi:10.1002/bjs.1800761110
-
Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60(6):441-446.
-
Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133-164. doi:10.1086/649554
-
Winbladh A, Gullstrand P, Svanvik J, et al. Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB (Oxford). 2009;11(3):183-193. doi:10.1111/j.1477-2574.2009.00052.x
-
Date RS, Kaushal M, Ramesh A. A review of the management of gallstone disease and its complications in pregnancy. Am J Surg. 2008;196(4):599-608. doi:10.1016/j.amjsurg.2008.01.015
-
Ansaloni L, Pisano M, Coccolini F, et al. 2016 WSES guidelines on acute calculous cholecystitis. World J Emerg Surg. 2016;11:25. doi:10.1186/s13017-016-0082-5
Last Updated: 2025-01-09 Quality Assessment: Gold Standard (54/56) - Comprehensive evidence-based content with 20 PubMed citations
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Clinical decisions should account for individual patient circumstances. Always consult appropriate specialists and refer to local guidelines.
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for acute cholecystitis?
Seek immediate emergency care if you experience any of the following warning signs: Gangrenous cholecystitis - necrotic wall with perforation risk, Perforation with biliary peritonitis, Sepsis or septic shock, Emphysematous cholecystitis - gas-forming organisms, Mirizzi syndrome - compression of common hepatic duct, Gallbladder empyema - pus-filled gallbladder, Acalculous cholecystitis in critically ill patients, Portal pyaemia with liver abscess.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Biliary Anatomy
- Gallstone Disease
Differentials
Competing diagnoses and look-alikes to compare.
- Acute Cholangitis
- Acute Pancreatitis
- Perforated Peptic Ulcer
Consequences
Complications and downstream problems to keep in mind.
- Biliary Peritonitis
- Bile Duct Injury