Thyroid Storm
Thyroid storm (thyrotoxic crisis) is a rare but life-threatening endocrine emergency characterized by severe, decompensa... MRCP exam preparation.
What matters first
Thyroid storm (thyrotoxic crisis) is a rare but life-threatening endocrine emergency characterized by severe, decompensa... MRCP exam preparation.
Hyperpyrexia (less than 40CC)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Hyperpyrexia (less than 40CC)
- Cardiovascular collapse
- Altered mental status progressing to coma
- Seizures
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Sepsis and Septic Shock
- Neuroleptic Malignant Syndrome
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
Thyroid storm (thyrotoxic crisis) is a rare but life-threatening endocrine emergency characterized by severe, decompensa... MRCP exam preparation.
Thyroid storm (thyrotoxic crisis) is an acute, severe, life-threatening exacerbation of thyrotoxicosis with multiorgan d... ACEM Primary Written, ACEM Primary V
1. Diagnose thyroid storm using Burch-Wartofsky Point Scale (≥45 = storm)... CICM Second Part exam preparation.
Clinical explanation and evidence
Thyroid Storm
1. Overview
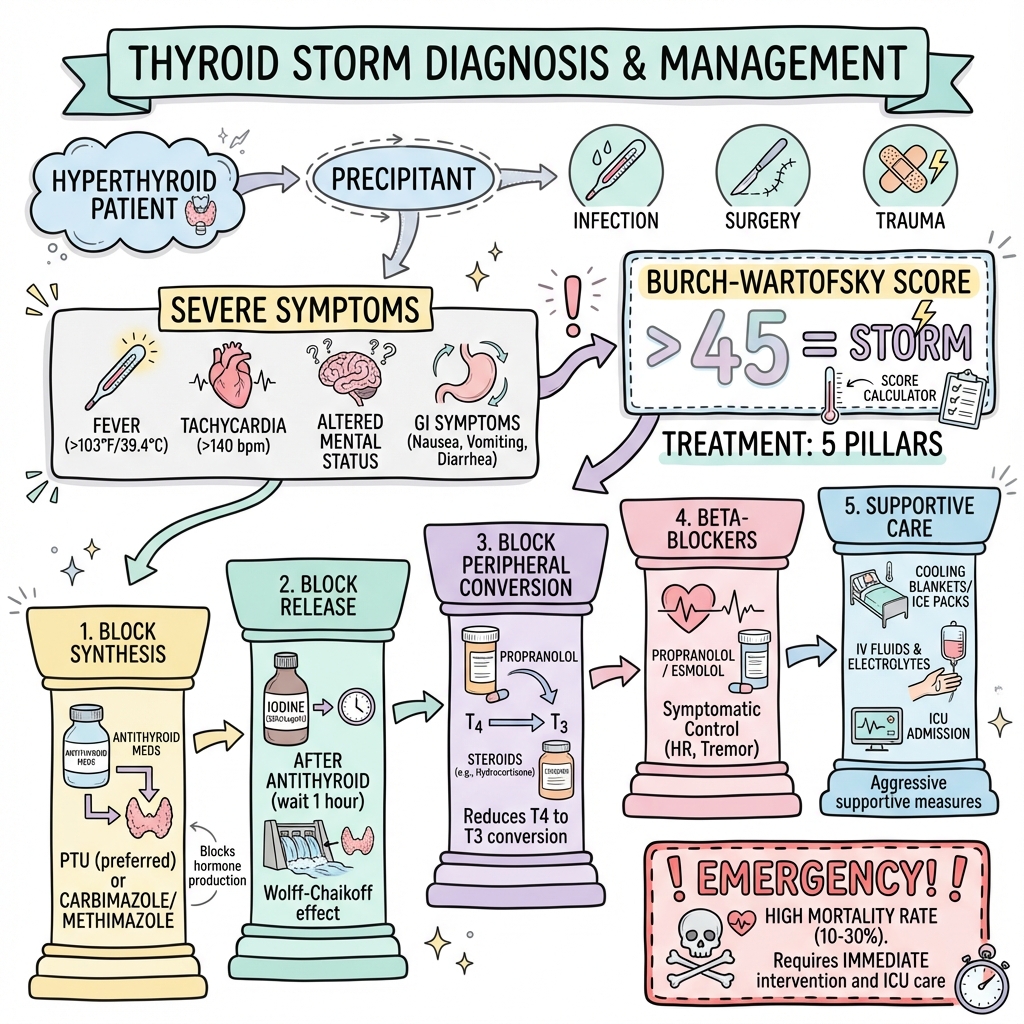
Thyroid storm (thyrotoxic crisis) is a rare but life-threatening endocrine emergency characterized by severe, decompensated thyrotoxicosis with multisystem dysfunction. It represents the extreme manifestation of hyperthyroidism, typically occurring in patients with underlying thyroid disease who experience a precipitating event such as infection, surgery, or trauma. The condition is distinguished from uncomplicated thyrotoxicosis by systemic decompensation affecting the cardiovascular, thermoregulatory, central nervous, and gastrointestinal systems. [1,2]
Despite modern intensive care management, thyroid storm remains associated with significant mortality, ranging from 10-30% even with appropriate treatment. [3,4] The diagnosis is fundamentally clinical, as thyroid hormone levels may not differ significantly between thyroid storm and uncomplicated thyrotoxicosis. The Burch-Wartofsky Point Scale is widely used to stratify patients, with scores ≥45 highly suggestive of thyroid storm. [5]
Management requires urgent recognition and aggressive multimodal therapy targeting five key mechanisms: blocking thyroid hormone synthesis, preventing thyroid hormone release, inhibiting peripheral conversion of T4 to T3, providing beta-adrenergic blockade, and treating the precipitating cause alongside supportive measures. [6,7]
2. Epidemiology
Thyroid storm is a rare complication of hyperthyroidism, occurring in approximately 1-2% of patients with thyrotoxicosis. [8] The condition affects predominantly females (female:male ratio approximately 3:1), reflecting the underlying gender distribution of thyroid disease. [9]
| Epidemiological Feature | Value | Source |
|---|---|---|
| Incidence in thyrotoxic patients | 1-2% | [8] |
| Mortality rate (treated) | 10-30% | [3,4] |
| Mortality rate (untreated) | > 90% | [1] |
| Mean age at presentation | 40-60 years | [9] |
| Female predominance | 3:1 | [9] |
| ICU admission requirement | > 80% | [10] |
Based on Japanese nationwide surveys, the incidence of thyroid storm is approximately 0.20 per 100,000 population per year. [2] Among hospitalized patients with thyrotoxicosis, thyroid storm develops in 3-10% of cases. [11]
Risk Factors
The development of thyroid storm requires both underlying hyperthyroidism (most commonly Graves' disease) and a precipitating event. Key risk factors include:
- Underlying thyroid disease: Graves' disease (60-80%), toxic multinodular goiter, toxic adenoma, iodine-induced thyrotoxicosis
- Inadequate treatment: Medication non-compliance, undiagnosed hyperthyroidism
- Advanced age: Older patients experience higher mortality
- Comorbidities: Heart failure, atrial fibrillation, coronary artery disease
Temporal Trends
Recent data suggest mortality rates have declined over the past two decades from 20-50% to 10-30%, attributed to improved recognition, earlier intervention, and advances in critical care management. [4,12] However, the condition remains a true medical emergency requiring immediate intensive care.
3. Aetiology and Pathophysiology
Aetiology
Thyroid storm typically occurs in patients with pre-existing hyperthyroidism exposed to a precipitating factor. The most common underlying causes include:
Primary Hyperthyroid Conditions (in order of frequency):
- Graves' disease (60-80%) [1]
- Toxic multinodular goiter (15-20%)
- Toxic adenoma (5-10%)
- Iodine-induced thyrotoxicosis (Jod-Basedow phenomenon)
- Excessive levothyroxine ingestion (rare)
Precipitating Factors (essential for storm development):
| Category | Specific Triggers |
|---|---|
| Infection (most common 20-50%) | Pneumonia, urinary tract infection, sepsis, COVID-19 [13] |
| Surgical stress | Thyroid surgery, non-thyroidal surgery, trauma |
| Iodine exposure | Radiocontrast media, amiodarone, iodinated antiseptics |
| Medication-related | Antithyroid drug withdrawal, aspirin displacing thyroid hormone from binding proteins |
| Cardiovascular events | Myocardial infarction, pulmonary embolism, congestive heart failure |
| Endocrine | Diabetic ketoacidosis, hypoglycemia |
| Obstetric | Pregnancy, labor, delivery, hyperemesis gravidarum [14] |
| Other | Radioactive iodine therapy, vigorous thyroid palpation, emotional stress |
Pathophysiology
The pathophysiology of thyroid storm is incompletely understood, as thyroid hormone levels (TSH, free T4, free T3) do not reliably distinguish storm from uncomplicated thyrotoxicosis. [15] Multiple mechanisms contribute to systemic decompensation:
1. Excessive Thyroid Hormone Effects
Thyroid hormones exert genomic and non-genomic effects on multiple organ systems:
- Cardiovascular system: Increased β-adrenergic receptor expression and sensitivity, enhanced cardiac contractility and heart rate, reduced systemic vascular resistance, increased cardiac output (may increase 50-300%)
- Metabolic effects: Increased basal metabolic rate (30-100% above normal), enhanced thermogenesis, protein catabolism, lipolysis
- Gastrointestinal system: Increased motility, enhanced hepatic metabolism
2. Catecholamine Hypersensitivity
Although circulating catecholamine levels are not elevated in thyroid storm, there is marked enhancement of adrenergic responsiveness:
- Upregulation of β-adrenergic receptors [16]
- Increased receptor sensitivity to catecholamines
- Potentiation of catecholamine effects on cardiac tissue
- Enhanced conversion of T4 to T3 under stress conditions
3. Relative Adrenal Insufficiency
Accelerated cortisol metabolism due to increased hepatic clearance may result in functional adrenal insufficiency despite normal or elevated baseline cortisol levels. [17] This contributes to cardiovascular collapse and inability to mount appropriate stress response.
4. Cytokine-Mediated Inflammatory Response
Emerging evidence suggests a systemic inflammatory response contributes to thyroid storm:
- Elevated pro-inflammatory cytokines (IL-6, TNF-α, IL-1β)
- Possible "cytokine storm" phenomenon similar to other critical illnesses
- Enhanced oxidative stress and endothelial dysfunction [18]
5. Decompensation Mechanisms
The transition from compensated thyrotoxicosis to thyroid storm involves:
- Loss of compensatory mechanisms (cardiac reserve, thermoregulation)
- Acute precipitating stress overwhelming adaptive capacity
- Progressive multi-organ dysfunction
- Positive feedback loops amplifying metabolic derangement
4. Clinical Presentation
Thyroid storm presents with exaggerated features of thyrotoxicosis accompanied by systemic decompensation. The clinical diagnosis relies on recognizing the constellation of findings across multiple organ systems.
Cardinal Features
Thermoregulatory Dysfunction
- Hyperpyrexia: Temperature typically > 38.5°C, often > 40°C [2]
- Profuse diaphoresis
- Heat intolerance (from antecedent history)
Cardiovascular Manifestations
- Sinus tachycardia (heart rate typically > 140 bpm)
- Atrial fibrillation (10-35% of cases) [19]
- High-output cardiac failure
- Widened pulse pressure
- Hyperdynamic precordium
- Cardiogenic shock (in severe cases, 1% develop cardiogenic shock) [20]
Central Nervous System Progressive spectrum of dysfunction:
- Agitation, restlessness, emotional lability (early)
- Confusion, delirium (intermediate)
- Psychosis
- Stupor
- Seizures
- Coma (late, grave prognostic sign)
Gastrointestinal System
- Nausea and vomiting (common)
- Diarrhea (frequent, may be profuse)
- Abdominal pain
- Hepatic dysfunction (elevated transaminases, jaundice in severe cases)
Clinical Examination Findings
| System | Examination Findings | Frequency |
|---|---|---|
| General | Fever, diaphoresis, agitation | > 90% |
| Cardiovascular | Tachycardia, wide pulse pressure, systolic flow murmur | > 95% |
| Respiratory | Tachypnea, pulmonary edema (if heart failure present) | 40-60% |
| Thyroid | Goiter (may be diffuse or nodular), thyroid bruit (Graves') | 70-90% |
| Ophthalmologic | Lid lag, lid retraction, exophthalmos (if Graves') | 30-50% |
| Neuromuscular | Tremor, hyperreflexia, proximal myopathy | 70-85% |
| Dermatologic | Warm, moist skin, pretibial myxedema (Graves'), onycholysis | Variable |
Burch-Wartofsky Point Scale
The Burch-Wartofsky Point Scale (BWPS) is the most widely used diagnostic scoring system for thyroid storm. [5] It incorporates thermoregulatory, cardiovascular, central nervous system, gastrointestinal-hepatic dysfunction, and precipitant factors.
Burch-Wartofsky Point Scale Components:
1. Thermoregulatory Dysfunction (Temperature °F/°C)
- 99-99.9°F / 37.2-37.7°C: 5 points
- 100-100.9°F / 37.8-38.2°C: 10 points
- 101-101.9°F / 38.3-38.8°C: 15 points
- 102-102.9°F / 38.9-39.3°C: 20 points
- 103-103.9°F / 39.4-39.9°C: 25 points
- ≥104°F / ≥40°C: 30 points
2. Central Nervous System Effects
- Absent: 0 points
- Mild (agitation): 10 points
- Moderate (delirium, psychosis, extreme lethargy): 20 points
- Severe (seizures, coma): 30 points
3. Gastrointestinal-Hepatic Dysfunction
- Absent: 0 points
- Moderate (diarrhea, nausea/vomiting, abdominal pain): 10 points
- Severe (unexplained jaundice): 20 points
4. Cardiovascular Dysfunction
Tachycardia (beats per minute):
- 99-109: 5 points
- 110-119: 10 points
- 120-129: 15 points
- 130-139: 20 points
- ≥140: 25 points
Atrial fibrillation: 10 points
Congestive heart failure:
- Absent: 0 points
- Mild (pedal edema): 5 points
- Moderate (bibasilar rales): 10 points
- Severe (pulmonary edema): 15 points
5. Precipitant History
- Present: 0 points
- Absent: 10 points
Score Interpretation:
- ≥45 points: Highly suggestive of thyroid storm
- 25-44 points: Impending thyroid storm
- less than 25 points: Thyroid storm unlikely
5. Differential Diagnosis
Thyroid storm must be distinguished from other conditions presenting with hypermetabolic state, fever, tachycardia, and altered mental status.
| Condition | Key Distinguishing Features | Diagnostic Tests |
|---|---|---|
| Sepsis/Septic Shock | Source of infection identifiable, positive cultures, elevated lactate, normal or low thyroid hormones | Blood cultures, procalcitonin, TFTs |
| Neuroleptic Malignant Syndrome | Recent antipsychotic use, muscular rigidity (lead-pipe), elevated CK, bradyreflexia | Medication history, CK, TFTs |
| Serotonin Syndrome | Recent serotonergic drug use, clonus, hyperreflexia, mydriasis, onset within 24 hours | Medication history, TFTs |
| Malignant Hyperthermia | Exposure to volatile anesthetics or succinylcholine, masseter muscle spasm, very high CK | Anesthetic history, CK, contracture testing |
| Phaeochromocytoma Crisis | Episodic symptoms, severe hypertension (often > 220/120), elevated catecholamines | Plasma/urine metanephrines, TFTs |
| Sympathomimetic Toxicity | Drug ingestion history (cocaine, amphetamines), mydriasis, often hypertensive | Urine drug screen, TFTs |
| Anticholinergic Toxicity | Dry skin and mucous membranes, urinary retention, dilated pupils, "mad as a hatter, red as a beet, dry as a bone" | Clinical diagnosis, TFTs |
| Infection (severe) | Focal infection signs, appropriate response to antimicrobials, normal thyroid function | Culture data, imaging, TFTs |
| Heat Stroke | Environmental exposure, rapid onset, absence of sweating in classic form | History, core temperature, TFTs |
Clinical Pearls for Differentiation
- Sweating patterns: Thyroid storm presents with profuse diaphoresis; anticholinergic toxicity and classic heat stroke present with dry skin
- Reflexes: Hyperreflexia in thyroid storm and serotonin syndrome; hyporeflexia/bradyreflexia in neuroleptic malignant syndrome
- Onset: Thyroid storm develops over days; serotonin syndrome develops within hours; NMS develops over days to weeks
- Thyroid examination: Goiter, bruit, or ophthalmopathy strongly suggest thyroid etiology
6. Investigations
Critical principle: Thyroid storm is a clinical diagnosis. Treatment should not be delayed while awaiting laboratory confirmation, as thyroid hormone levels do not reliably distinguish storm from uncomplicated thyrotoxicosis.
Essential Initial Investigations
Thyroid Function Tests
- TSH: Suppressed (less than 0.01 mIU/L in most cases) [15]
- Free T4: Elevated (typically markedly, but degree does not correlate with storm severity)
- Free T3: Elevated (more metabolically active form)
- Note: Absolute levels do not distinguish storm from severe uncomplicated thyrotoxicosis
Identify Precipitating Cause
- Infection workup: Complete blood count, blood cultures, urinalysis, urine culture, chest X-ray
- Cardiac evaluation: ECG (atrial fibrillation, ischemia), troponin, NT-proBNP
- Metabolic panel: Glucose (may show hyperglycemia), electrolytes, renal function
- Liver function: Transaminases (often elevated), bilirubin (may be elevated in severe cases)
Additional Investigations
| Investigation | Expected Findings | Clinical Significance |
|---|---|---|
| Complete Blood Count | Leukocytosis (left shift if infection), anemia | Identify infection, assess severity |
| Arterial Blood Gas | Respiratory alkalosis (early), lactic acidosis (severe cases) | Assess metabolic status, organ perfusion |
| Calcium | Hypercalcemia (mild, 10-15% of cases) | Increased bone turnover |
| Magnesium | Hypomagnesemia | May contribute to arrhythmias |
| Creatine Kinase | Elevated (rhabdomyolysis in severe cases) | Muscle breakdown, renal risk |
| Cortisol | Normal to elevated (but inadequate for stress level) | Relative adrenal insufficiency |
| Thyroid Antibodies | TSH receptor antibodies (if Graves' disease) | Identify underlying etiology |
| Imaging | Thyroid ultrasound, radioiodine uptake (NOT in acute setting) | Determine underlying thyroid pathology (after stabilization) |
Diagnostic Approach
Emergency Department/ICU Initial Assessment (First 30-60 minutes):
-
Immediate bedside: Vital signs (including temperature), cardiac monitoring, pulse oximetry
-
Urgent laboratory (stat processing):
- TSH, free T4, free T3
- Complete blood count with differential
- Comprehensive metabolic panel
- Liver function tests
- Blood cultures (if febrile)
- Troponin, NT-proBNP
- Arterial blood gas
-
Calculate Burch-Wartofsky score based on clinical presentation
-
Initiate treatment immediately if clinical suspicion high (score ≥25), do NOT wait for thyroid function results
Pitfalls in Diagnosis:
- Non-thyroidal illness syndrome: Critically ill patients may have low T3 and normal/low T4 despite low TSH—this represents sick euthyroid syndrome, NOT thyroid storm
- Subclinical hyperthyroidism: Low TSH with normal T4/T3 does NOT cause thyroid storm
- Assay interference: Biotin supplementation can interfere with thyroid function assays; heterophile antibodies may cause spurious results
7. Management
Thyroid storm management requires immediate, aggressive, multimodal therapy in an intensive care setting. Treatment is initiated based on clinical suspicion without waiting for laboratory confirmation.
Immediate Resuscitation (First Hour)
ABCDE Approach:
- Airway: Assess and secure if altered mental status/impending respiratory failure
- Breathing: Supplemental oxygen, consider mechanical ventilation if respiratory failure
- Circulation: Large-bore IV access, aggressive fluid resuscitation (may require 3-5L in first 24 hours due to increased insensible losses)
- Disability: Assess GCS, monitor for seizures
- Exposure: Cooling measures for hyperpyrexia
Supportive Care:
- ICU admission: Mandatory for all cases of thyroid storm
- Continuous cardiac monitoring: Detect arrhythmias, monitor heart rate response
- Temperature management: Aggressive cooling (paracetamol, cooling blankets, ice packs to groin/axillae). Avoid aspirin (displaces thyroid hormone from binding proteins) [7]
- Fluid resuscitation: Isotonic crystalloid, guided by hemodynamic monitoring
- Nutritional support: High caloric intake (may require 3000-4000 kcal/day)
Specific Pharmacological Therapy: The Five-Step Protocol
Treatment targets five distinct mechanisms. CRITICAL TIMING: Antithyroid drugs MUST be given BEFORE iodine (at least 1 hour prior) to prevent iodine-induced hormone synthesis. [6,7]
Step 1: Block Thyroid Hormone Synthesis (Thionamides)
First-line: Propylthiouracil (PTU)
- Dose: 200-250mg orally or via nasogastric tube every 4-6 hours (loading dose 500-1000mg) [21]
- Advantages: Also blocks peripheral conversion of T4 to T3 (Type 1 deiodinase inhibition)
- Disadvantages: Hepatotoxicity risk, shorter half-life requiring frequent dosing
- Administration: Oral, rectal (if GI dysfunction), or nasogastric tube
- No IV formulation available
Alternative: Methimazole (MMI)
- Dose: 20-30mg orally every 6 hours (loading dose 60-100mg) [21]
- Advantages: Longer half-life, less hepatotoxic than PTU, more potent per mg
- Disadvantages: Does NOT block peripheral conversion
- Recent evidence: Large retrospective study showed no mortality difference between PTU and MMI in critically ill thyroid storm patients [22]
- Pregnancy consideration: MMI contraindicated in first trimester (teratogenic); PTU preferred
Step 2: Block Thyroid Hormone Release (Iodine)
TIMING CRITICAL: Give at least 1 hour AFTER thionamides to prevent iodine from serving as substrate for new hormone synthesis (Wolff-Chaikoff effect must be established first). [6]
Lugol's Iodine (preferred)
- Dose: 5-10 drops (0.25-0.5mL) orally or via NGT every 6-8 hours
- Concentration: 5% iodine + 10% potassium iodide
- Mechanism: Inhibits thyroid hormone release (Wolff-Chaikoff effect), reduces thyroid vascularity
Alternatives:
- Saturated solution of potassium iodide (SSKI): 2-5 drops every 6 hours
- Iopanoic acid or sodium ipodate (oral cholecystographic agents): 0.5-1g daily (also blocks T4 to T3 conversion; not available in many countries)
- IV iodinated contrast (if patient cannot take oral): Sodium ipodate 1g daily
Contraindications: Iodine allergy (rare), amiodarone-induced thyrotoxicosis type 2
Step 3: Block Peripheral Conversion of T4 to T3
Multiple agents contribute to blocking peripheral conversion:
Propranolol (preferred beta-blocker)
- Blocks Type 1 deiodinase in addition to beta-blockade
- Dose for conversion blockade: Higher doses needed (see Step 4)
Corticosteroids (also provide adrenal support)
- Hydrocortisone: 100mg IV every 8 hours [17]
- Dexamethasone: 2mg IV every 6 hours (alternative)
- Dual mechanism: Blocks T4 to T3 conversion + treats relative adrenal insufficiency
- Duration: Continue until clinical improvement, then taper
Cholestyramine (adjunctive)
- Dose: 4g orally 3-4 times daily
- Mechanism: Bile acid sequestrant that interrupts enterohepatic recirculation of thyroid hormones [23]
- Use: Refractory cases or when other therapies contraindicated
Step 4: Beta-Adrenergic Blockade
Essential for controlling cardiovascular manifestations and sympathetic overactivity.
Propranolol (first-line)
- IV route (preferred in ICU):
- "Loading: 1-2mg IV over 10 minutes, may repeat every 10-15 minutes until heart rate less than 100 bpm [24]"
- "Maintenance: 1-10mg IV every 4 hours OR continuous infusion"
- Oral route:
- 40-80mg every 4-6 hours (if patient can take oral, GI absorption reliable)
- Titrate to heart rate control
- Advantages: Also blocks peripheral T4 to T3 conversion, extensive clinical experience
- Target: Heart rate 80-100 bpm
Caution with Beta-Blockers:
- Cardiovascular collapse risk: Reports of cardiac arrest following propranolol administration in thyroid storm, likely due to acute negative inotropic effects in maximally stressed myocardium [25]
- Recommended approach: Cautious dose escalation with continuous monitoring, have resuscitative equipment immediately available
- Recent evidence: Beta-1 selective agents (esmolol, landiolol) may have similar efficacy with potentially lower risk of cardiac arrest [24]
Alternative Beta-Blockers:
Esmolol (cardioselective)
- Dose: Loading 250-500 mcg/kg IV over 1 minute, then 50-100 mcg/kg/min infusion
- Advantages: Ultra-short half-life (9 minutes), easily titrated, rapidly reversible
- Disadvantages: Does not block T4 to T3 conversion, requires continuous infusion
- Use: Preferred if hemodynamic instability, heart failure, or concern for cardiovascular collapse [24]
Landiolol (cardioselective, ultra-short-acting)
- Used in Japan, not available in all countries
- Similar benefits to esmolol
If Beta-Blockers Contraindicated:
- Diltiazem: 0.25mg/kg IV bolus, then 5-15mg/hr infusion (for heart rate control only, does not address adrenergic symptoms)
- Reserpine: 1-5mg IM every 4-6 hours (depletes catecholamines; rarely used)
- Guanethidine: 1-2mg/kg/day orally (peripheral adrenergic blocker; rarely used)
Step 5: Treat Precipitating Cause and Provide Supportive Care
Identify and Treat Precipitant:
- Infection: Broad-spectrum antibiotics after cultures (most common precipitant)
- Cardiac events: Anticoagulation for AF, optimize heart failure management
- Other: Address DKA, discontinue offending medications, etc.
Supportive Measures:
- Fluid resuscitation: 3-5L crystalloid in first 24 hours (increased insensible losses)
- Electrolyte replacement: Magnesium, potassium, phosphate as needed
- Nutritional support: High-calorie diet (increased metabolic demand)
- Cooling measures: Target temperature less than 38°C
- Avoid: Aspirin (displaces thyroid hormone from binding proteins), large doses of acetaminophen alone may be insufficient
Refractory Thyroid Storm: Advanced Therapies
For patients not responding to conventional therapy within 24-48 hours, consider advanced modalities:
Therapeutic Plasma Exchange (Plasmapheresis)
- Indication: Refractory thyroid storm despite maximal medical therapy [26]
- Mechanism: Direct removal of circulating thyroid hormones (T4, T3) and thyroid-stimulating antibodies
- Protocol: Daily sessions until clinical improvement (typically 3-8 sessions)
- Evidence: Multiple case reports/series showing rapid clinical improvement and hormone reduction
- Complications: Vascular access, coagulopathy, hypocalcemia, infection
Emergency Thyroidectomy
- Indication: Refractory thyroid storm, contraindication to medical therapy, massive goiter causing airway compromise
- Timing: Only when hemodynamically stable enough to tolerate anesthesia (or on ECMO support) [27]
- Preparation: Optimize with medical therapy for 24-48 hours if possible, consider plasmapheresis pre-operatively
- Risk: Very high surgical morbidity/mortality in acutely ill patients
- Evidence: Case series show success but require experienced thyroid surgeon and multidisciplinary team
- Post-operative: Monitor for hypocalcemia, recurrent laryngeal nerve injury, ongoing critical illness
Extracorporeal Membrane Oxygenation (ECMO)
- Indication: Refractory cardiovascular collapse, bridge to definitive therapy
- Use: Rare, case reports of successful bridge to emergency thyroidectomy [27]
Other Adjunctive Therapies:
- Lithium carbonate: 300mg orally 2-3 times daily (blocks thyroid hormone release; rarely used due to toxicity)
- Percutaneous coronary intervention/mechanical support: If concurrent acute coronary syndrome or cardiogenic shock
Special Populations
Pregnancy:
- PTU preferred over methimazole in all trimesters for thyroid storm
- Beta-blockers: Propranolol considered safe, use lowest effective dose
- Iodine: Generally avoided in pregnancy but acceptable in life-threatening thyroid storm
- Corticosteroids: Considered safe
- Delivery planning: Multidisciplinary approach, avoid cesarean section unless obstetric indication
Elderly:
- Lower doses of beta-blockers due to increased cardiac sensitivity
- Higher risk of cardiac complications
- Careful fluid balance (risk of fluid overload)
Concurrent Heart Failure:
- Cautious beta-blocker use (start low, go slow)
- Consider cardioselective agents (esmolol)
- Aggressive diuresis as needed
- Early cardiology consultation
8. Complications
Thyroid storm results in multiorgan dysfunction. Recognition and management of complications is essential.
| Complication | Incidence | Management | Prevention |
|---|---|---|---|
| Atrial Fibrillation | 10-35% | Rate control (beta-blockers preferred), anticoagulation (CHA2DS2-VASc score), electrical cardioversion if unstable | Adequate beta-blockade |
| Acute Heart Failure | 15-30% | Diuretics, afterload reduction, treat underlying thyrotoxicosis, mechanical support if needed | Judicious fluid management, early heart failure treatment |
| Cardiogenic Shock | 1-5% | Inotropes/pressors (with caution), mechanical circulatory support, ECMO, urgent thyroidectomy consideration [20] | Aggressive early treatment |
| Cardiovascular Collapse | 5-10% | Resuscitation, pressors, consider esmolol vs propranolol | Careful beta-blocker dosing [25] |
| Acute Kidney Injury | 10-20% | Fluid resuscitation, avoid nephrotoxins, renal replacement therapy if severe | Adequate hydration |
| Hepatic Dysfunction | 30-50% | Supportive care, treat underlying cause, avoid hepatotoxic medications | Monitor LFTs, minimize PTU if severe hepatotoxicity |
| Rhabdomyolysis | 5-10% | Aggressive hydration, alkalinization of urine, monitor CK and renal function | Cooling, adequate hydration |
| Disseminated Intravascular Coagulation (DIC) | 5-15% | Treat underlying cause, supportive care, blood product replacement | Early aggressive treatment of thyroid storm [28] |
| Seizures | less than 5% | Benzodiazepines, antiepileptics, cooling, treat electrolyte abnormalities | Temperature control, electrolyte balance |
| Respiratory Failure | 10-20% | Supplemental oxygen, mechanical ventilation if needed | Early respiratory support |
| Multiorgan Dysfunction Syndrome (MODS) | Variable | Intensive care support, treat all organ dysfunctions | Early recognition and aggressive treatment |
High-Risk Complications Requiring Special Attention
Cardiovascular Collapse Post-Beta-Blocker Administration: A well-documented but rare complication where patients develop sudden cardiac arrest following propranolol administration. [25] Risk factors include severe thyrotoxicosis, pre-existing cardiac dysfunction, and high doses. The proposed mechanism involves acute negative inotropy in an already maximally stressed myocardium dependent on high sympathetic tone. Preventive strategies include:
- Start with lower doses of beta-blocker
- Consider cardioselective agents (esmolol) in high-risk patients
- Have resuscitative equipment immediately available
- Consider echocardiography to assess baseline cardiac function
Disseminated Intravascular Coagulation: Recent single-center study identified DIC as a frequent (33%) and critical complication of thyroid storm, associated with higher mortality. [28] Proposed mechanisms include endothelial injury from hyperthyroidism, increased procoagulant factors, and systemic inflammation. Monitor coagulation parameters closely.
9. Prognosis
Short-term Outcomes
Mortality:
- Overall mortality: 10-30% with treatment [3,4]
- Untreated mortality: > 90% [1]
- Mortality has decreased from 20-50% historically to 10-30% in modern era [12]
Factors Associated with Increased Mortality:
| Factor | Odds Ratio/Relative Risk |
|---|---|
| Age > 60 years | 2.5-3.0 |
| Burch-Wartofsky score > 60 | 3-4 |
| Presence of heart failure | 2-3 |
| Development of DIC | 4-5 |
| Multiorgan dysfunction | 5-10 |
| Need for mechanical ventilation | 3-5 |
| Cardiogenic shock | 5-8 |
Recovery Time:
- Clinical improvement typically begins 24-48 hours after initiation of therapy
- Heart rate normalizes within 24-72 hours in most cases
- Temperature normalizes within 24-48 hours
- Mental status improvement may lag behind biochemical improvement [29]
- Full recovery may take 1-2 weeks
Long-term Outcomes
Patients who survive thyroid storm require definitive management of underlying hyperthyroidism to prevent recurrence:
Definitive Therapy Options:
- Radioactive iodine (RAI) ablation (most common after stabilization)
- Total thyroidectomy (especially if prior storm or contraindication to RAI)
- Long-term antithyroid drug therapy (least preferred due to recurrence risk)
Post-Storm Management:
- Continue antithyroid medication until definitive therapy completed
- Gradual withdrawal of supportive medications
- Address underlying precipitant (e.g., treat chronic infection)
- Patient education on medication compliance
- Plan for definitive thyroid ablation or surgery (typically 3-6 months post-storm)
10. Prevention and Screening
Primary Prevention
High-Risk Patient Identification:
- Patients with known hyperthyroidism planning surgery
- Graves' disease patients with poor compliance
- Patients with toxic multinodular goiter or toxic adenoma
Pre-operative Optimization:
- Achieve euthyroid state before elective thyroid surgery
- Beta-blockade for all hyperthyroid patients undergoing surgery
- Consider stress-dose corticosteroids peri-operatively
Patient Education:
- Importance of medication compliance
- Recognition of early warning signs (worsening tremor, palpitations, fever)
- Avoid iodinated contrast unless essential (pre-medicate with thionamides if necessary)
- Prompt treatment of intercurrent illnesses
Screening Recommendations
No specific screening programs exist for thyroid storm prevention, but screening for hyperthyroidism is important in:
- Atrial fibrillation (especially new-onset)
- Unexplained weight loss or anxiety
- Family history of thyroid disease
- Autoimmune conditions
11. Key Guidelines
American Thyroid Association (ATA) Guidelines 2016
Key Recommendations for Thyroid Storm Management: [30]
- Diagnosis based on clinical criteria and scoring systems (Burch-Wartofsky)
- Initiate treatment immediately based on clinical suspicion
- Multi-modal therapy targeting synthesis, release, and peripheral conversion
- ICU-level monitoring required
- Propylthiouracil preferred over methimazole (historical recommendation)
- Iodine administration at least 1 hour after thionamide
- Beta-blockade essential (propranolol preferred historically)
- Glucocorticoid therapy for all patients
- Identify and treat precipitating cause
- Consider plasmapheresis or thyroidectomy for refractory cases
Note: Recent evidence (2023) suggests methimazole may be equivalent to PTU in critically ill thyroid storm patients, challenging traditional preference. [22]
Japanese Thyroid Association Diagnostic Criteria (2012)
More conservative diagnostic criteria than Burch-Wartofsky, emphasizing combination of thyrotoxicosis with specific organ dysfunction criteria (CNS, cardiac, GI, fever). [2] Useful as complementary diagnostic approach.
European Thyroid Association Guidelines
Support multimodal therapy approach similar to ATA, with emphasis on individualized treatment based on patient factors and local drug availability.
12. Common Examination Questions
Written Examination (MCQ/SAQ)
High-Yield Questions:
-
"A 45-year-old woman presents with fever (40°C), heart rate 150 bpm, confusion, and profuse sweating. She has known Graves' disease and was recently treated for pneumonia. What is your immediate management?"
-
"Why must antithyroid drugs be administered before iodine in thyroid storm management?"
-
"Calculate the Burch-Wartofsky score for a patient with: Temperature 39.5°C, heart rate 145, atrial fibrillation, severe delirium, diarrhea, recent trauma."
-
"A patient with thyroid storm develops cardiac arrest shortly after receiving IV propranolol. What is the mechanism and how could this have been prevented?"
-
"What are the five mechanisms targeted in thyroid storm pharmacotherapy?"
Clinical Examination (OSCE/PACES)
Scenario: ICU Patient with Suspected Thyroid Storm
You are called to ICU to review a 52-year-old woman admitted 2 hours ago with fever, confusion, and rapid heart rate. Examination reveals temperature 39.8°C, heart rate 155 regular, BP 145/65, profuse sweating, tremor, diffuse goiter with bruit, and agitation.
Expected approach:
- Recognition: "This patient has features suggestive of thyroid storm"
- Assessment: Calculate Burch-Wartofsky score (verbalize components)
- Immediate management plan following 5-step protocol
- Initiate investigations while starting treatment
- Explain critical timing (thionamide BEFORE iodine)
- Identify and treat precipitant
Viva Points
Opening Statement for Oral Examination:
"Thyroid storm is a rare but life-threatening endocrine emergency characterized by severe thyrotoxicosis with systemic decompensation affecting cardiovascular, thermoregulatory, central nervous, and gastrointestinal systems. It occurs in 1-2% of patients with hyperthyroidism, typically precipitated by infection, surgery, or other physiological stress. Mortality remains 10-30% despite treatment. Diagnosis is clinical using the Burch-Wartofsky Point Scale, with scores ≥45 highly suggestive of storm. Treatment is immediate and multimodal, targeting five mechanisms: blocking thyroid hormone synthesis with thionamides, preventing release with iodine administered one hour after thionamides, inhibiting peripheral conversion with steroids and propranolol, providing beta-blockade, and treating the precipitating cause."
Essential Facts to Remember:
- Burch-Wartofsky scoring: ≥45 = storm, 25-44 = impending, less than 25 = unlikely
- Mortality: 10-30% treated, > 90% untreated
- Critical timing: Thionamide BEFORE iodine (minimum 1-hour gap)
- Five-step protocol: Synthesis block → Release block → Conversion block → Beta-blockade → Supportive care
- PTU dosing: 200-250mg Q4-6H (500-1000mg loading)
- Propranolol dosing: 1-2mg IV Q10-15min or 40-80mg PO Q4-6H
- Hydrocortisone: 100mg IV Q8H
- Iodine timing: 1 hour after thionamide, 5-10 drops Lugol's Q6-8H
- Precipitants: Infection most common, also surgery, iodine, DKA, drugs
- Refractory management: Plasmapheresis, emergency thyroidectomy
Common Examiner Follow-up Questions:
- "Why doesn't TSH level alone diagnose thyroid storm?" → Levels don't distinguish storm from uncomplicated thyrotoxicosis; diagnosis is clinical
- "Why use both PTU and propranolol rather than just one?" → Different mechanisms: PTU blocks synthesis and T4→T3 conversion; propranolol provides adrenergic blockade and also blocks conversion
- "When would you consider emergency thyroidectomy?" → Refractory storm despite maximal medical therapy including plasmapheresis, contraindication to medical management, massive goiter with airway compromise
- "What is the risk of beta-blockers in thyroid storm?" → Cardiovascular collapse/cardiac arrest due to acute negative inotropic effect in stressed myocardium; use cautiously with continuous monitoring
Common Mistakes
Mistakes That Fail Candidates:
❌ Waiting for thyroid function tests before initiating treatment → Thyroid storm is a clinical diagnosis; treatment must start immediately
❌ Giving iodine before or simultaneously with thionamides → Iodine without thionamide blockade provides substrate for new hormone synthesis
❌ Using aspirin for fever control → Aspirin displaces thyroid hormone from binding proteins, worsening thyrotoxicosis
❌ Failing to calculate Burch-Wartofsky score → Objective scoring improves diagnostic accuracy and risk stratification
❌ Administering propranolol rapidly without monitoring → Risk of cardiovascular collapse and cardiac arrest
❌ Missing the precipitating cause → Failing to identify and treat infection, DKA, or other precipitant leads to treatment failure
❌ Inadequate dose or frequency of medications → Subtherapeutic doses (e.g., PTU Q12H instead of Q4-6H) ineffective
❌ Forgetting corticosteroids → Relative adrenal insufficiency contributes to decompensation
Model Answer
Q: Describe your approach to managing a patient with suspected thyroid storm.
A: "I would approach this as a life-threatening endocrine emergency requiring immediate ICU admission and multimodal therapy.
Initial Assessment (ABCDE approach): First, I would ensure airway patency, provide supplemental oxygen, establish large-bore IV access, initiate continuous cardiac monitoring, and begin aggressive fluid resuscitation. I would perform a rapid clinical examination focusing on vital signs (temperature, heart rate, blood pressure), mental status, thyroid examination, and identification of potential precipitants.
Diagnostic Evaluation: I would calculate the Burch-Wartofsky Point Scale based on temperature, tachycardia, CNS symptoms, GI symptoms, cardiac dysfunction, and precipitant presence. A score ≥45 is highly suggestive of thyroid storm. Simultaneously, I would order urgent investigations including TSH, free T4, free T3, complete blood count, comprehensive metabolic panel, liver function tests, blood cultures, ECG, and chest X-ray. However, I would NOT wait for these results before initiating treatment.
Immediate Treatment (Five-Step Protocol):
Step 1 - Block synthesis: Propylthiouracil 500-1000mg loading dose, then 200-250mg orally or via NGT every 4-6 hours. PTU is preferred as it also blocks peripheral T4 to T3 conversion.
Step 2 - Block release: Lugol's iodine 5-10 drops every 6-8 hours, administered at least 1 hour AFTER the thionamide to prevent iodine serving as substrate for new hormone synthesis.
Step 3 - Block peripheral conversion: Hydrocortisone 100mg IV every 8 hours, which blocks T4 to T3 conversion and treats relative adrenal insufficiency.
Step 4 - Beta-adrenergic blockade: Propranolol 1-2mg IV over 10 minutes, repeated every 10-15 minutes until heart rate less than 100 bpm, with continuous cardiac monitoring due to cardiovascular collapse risk. Alternatively, esmolol infusion if concern for cardiac decompensation.
Step 5 - Treat precipitant and supportive care: Identify and treat infection with broad-spectrum antibiotics, provide aggressive cooling with paracetamol and cooling blankets (avoiding aspirin which displaces thyroid hormone from binding proteins), correct electrolyte abnormalities, and provide nutritional support.
Monitoring and Escalation: I would reassess clinical response every 4-6 hours. If refractory to medical management after 24-48 hours, I would consider therapeutic plasmapheresis to directly remove circulating thyroid hormones. In extreme cases unresponsive to all medical measures, emergency thyroidectomy may be necessary, though this carries very high surgical risk.
This approach follows current ATA guidelines and targets all five critical mechanisms to rapidly reduce thyroid hormone levels and effects."
References
-
Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am. 1993;22(2):263-277. PMID: 8325286
-
Akamizu T, Satoh T, Isozaki O, et al. Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys. Thyroid. 2012;22(7):661-679. doi:10.1089/thy.2011.0334
-
Bourcier S, Coutrot M, Kimmoun A, et al. Thyroid Storm in the ICU: A Retrospective Multicenter Study. Crit Care Med. 2020;48(1):83-90. doi:10.1097/CCM.0000000000004078
-
Kornelius E, Chang KL, Yang YS, et al. Epidemiology and factors associated with mortality of thyroid storm in Taiwan: a nationwide population-based study. Intern Emerg Med. 2021;16(3):601-607. doi:10.1007/s11739-020-02445-6
-
Burch HB, Wartofsky L. Burch-Wartofsky Point Scale for diagnosing thyroid storm. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000. (Established 1993)
-
Chiha M, Samarasinghe S, Kabaker AS. Thyroid storm: an updated review. J Intensive Care Med. 2015;30(3):131-140. doi:10.1177/0885066613498053
-
Idrose AM. Acute and emergency care for thyrotoxicosis and thyroid storm. Acute Med Surg. 2015;2(3):147-157. doi:10.1002/ams2.104
-
Farooqi S, Raj S, Koyfman A, Long B. High risk and low prevalence diseases: Thyroid storm. Am J Emerg Med. 2023;69:127-135. doi:10.1016/j.ajem.2023.03.035
-
Akamizu T. Thyroid Storm: A Japanese Perspective. Thyroid. 2018;28(1):32-40. doi:10.1089/thy.2017.0243
-
Bourcier S, Coutrot M, Kimmoun A, et al. Thyroid Storm in the ICU: A Retrospective Multicenter Study. Crit Care Med. 2020;48(1):83-90.
-
Abisad DA, Glenn Lecea EM, Ballesteros AM, et al. Thyroid storm in pediatrics: a systematic review. J Pediatr Endocrinol Metab. 2023;36(3):225-233. doi:10.1515/jpem-2022-0309
-
Elendu C, Amaechi DC, Amaechi EC, et al. Diagnostic criteria and scoring systems for thyroid storm: An evaluation of their utility - comparative review. Medicine (Baltimore). 2024;103(13):e37396. doi:10.1097/MD.0000000000037396
-
Rao AN, Al-Ward RY, Gaba R. Thyroid Storm in a Patient With COVID-19. AACE Clin Case Rep. 2021;7(6):360-362. doi:10.1016/j.aace.2021.06.011
-
Zimmerman CF, Ilstad-Minnihan AB, Bruggeman BS, et al. Thyroid Storm Caused by Hyperemesis Gravidarum. AACE Clin Case Rep. 2022;8(3):124-127. doi:10.1016/j.aace.2021.12.005
-
Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10):1343-1421.
-
Dietrich JW. Thyroid storm. Med Klin Intensivmed Notfmed. 2012;107(6):448-453. doi:10.1007/s00063-012-0113-2
-
Klubo-Gwiezdzinska J, Wartofsky L. Thyroid emergencies. Med Clin North Am. 2012;96(2):385-403.
-
Elmenyar E, Aoun S, Al Saadi Z, et al. Data Analysis and Systematic Scoping Review on the Pathogenesis and Modalities of Treatment of Thyroid Storm Complicated with Myocardial Involvement and Shock. Diagnostics (Basel). 2023;13(19):3028. doi:10.3390/diagnostics13193028
-
Pink K, Yee AC, Ha ET, et al. Risk factors for cardiogenic shock in thyroid storm: a retrospective and case-series study. Future Cardiol. 2023;19(12):605-613. doi:10.2217/fca-2023-0043
-
Pink K, Yee AC, Ha ET, et al. Risk factors for cardiogenic shock in thyroid storm. Future Cardiol. 2023;19(12):605-613.
-
Lee SY, Modzelewski KL, Law AC, et al. Comparison of Propylthiouracil vs Methimazole for Thyroid Storm in Critically Ill Patients. JAMA Netw Open. 2023;6(4):e238655. doi:10.1001/jamanetworkopen.2023.8655
-
Lee SY, Modzelewski KL, Law AC, Walkey AJ, Pearce EN, Bosch NA. Comparison of Propylthiouracil vs Methimazole for Thyroid Storm in Critically Ill Patients. JAMA Netw Open. 2023;6(4):e238655.
-
Kruithoff ML, Gigliotti BJ. Thyroid Emergencies: A Narrative Review. Endocr Pract. 2025;31(10):1310-1318. doi:10.1016/j.eprac.2025.06.010
-
Matsuo Y, Jo T, Watanabe H, et al. Clinical Efficacy of Beta-1 Selective Beta-Blockers Versus Propranolol in Patients With Thyroid Storm: A Retrospective Cohort Study. Crit Care Med. 2024;52(7):1077-1086. doi:10.1097/CCM.0000000000006285
-
Dalan R, Leow MK. Cardiovascular collapse associated with beta blockade in thyroid storm. Exp Clin Endocrinol Diabetes. 2007;115(6):392-396. doi:10.1055/s-2007-971065
-
Wyble AJ, Moore SC, Yates SG. Weathering the storm: A case of thyroid storm refractory to conventional treatment benefiting from therapeutic plasma exchange. J Clin Apher. 2018;33(6):678-681. doi:10.1002/jca.21658
-
Koh H, Kaushik M, Loh JK, Chng CL. Plasma exchange and early thyroidectomy in thyroid storm requiring extracorporeal membrane oxygenation. Endocrinol Diabetes Metab Case Rep. 2019;2019(1):1-6. doi:10.1530/EDM-19-0051
-
Hoshiyama A, Hayashi A, Taguchi T, et al. Disseminated intravascular coagulation as a frequent and critical complication of thyroid storm: a single-center retrospective survey. Endocr J. 2025;72(6):719-726. doi:10.1507/endocrj.EJ24-0542
-
Evans M, Prince G, Majety P. A Case of Refractory Thyroid Storm Despite Correction of Peripheral Thyroid Hormone Levels. JCEM Case Rep. 2024;2(10):luae179. doi:10.1210/jcemcr/luae179
-
Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016;26(10):1343-1421. doi:10.1089/thy.2016.0229
Last Updated: 2026-01-05
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for thyroid storm?
Seek immediate emergency care if you experience any of the following warning signs: Hyperpyrexia (less than 40CC), Cardiovascular collapse, Altered mental status progressing to coma, Seizures, Acute heart failure, Atrial fibrillation with rapid ventricular response.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Sepsis and Septic Shock
- Neuroleptic Malignant Syndrome
- Serotonin Syndrome
- Phaeochromocytoma Crisis
Consequences
Complications and downstream problems to keep in mind.