EM · Toxicology and environmental emergencies
Iron poisoning
Also known as Iron toxicity · Ferrous sulphate overdose · Acute iron ingestion · Elemental iron poisoning · Desferrioxamine-responsive iron overdose
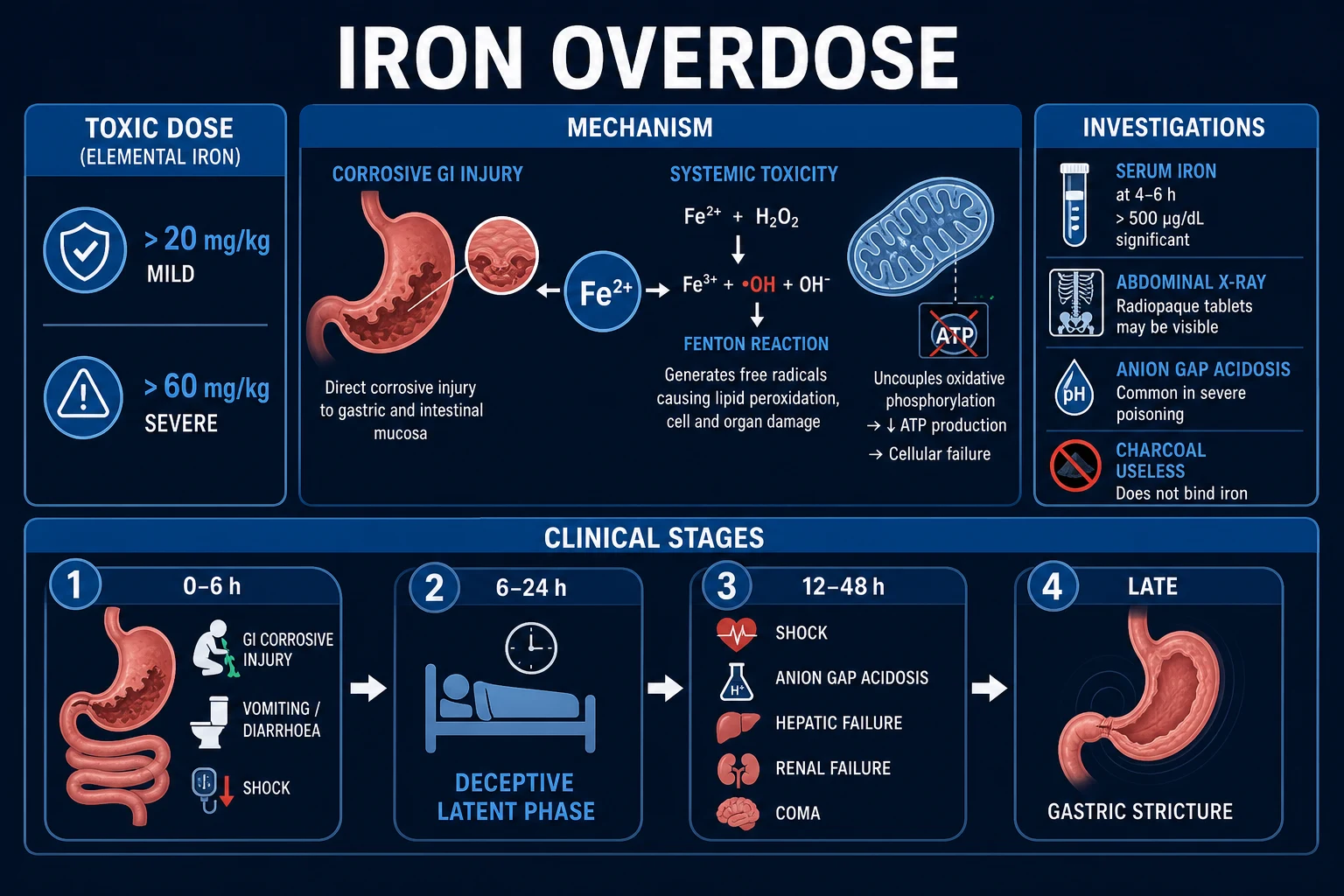
Iron poisoning — the heavy-metal overdose whose lethality rides on a single pharmacological concept: the body has no excretory route for free iron, so any dose that overwhelms transferrin's binding capacity releases catalytic free iron that drives free-radical lipid peroxidation of mitochondrial membranes. The clinical course unfolds in five stereotyped stages the Fellowship candidate must recite: gastrointestinal (nausea, vomiting, haematemesis, diarrhoea, 0 to 6 hours), quiescent (apparent recovery, 6 to 24 hours — the lethal trap), shock (distributive shock with capillary leak and metabolic acidosis, 12 to 24 hours), hepatotoxicity (centrilobular necrosis from mitochondrial free-radical injury, 1 to 3 days), and gastrointestinal obstruction (corrosive scarring with pyloric or intestinal stricture, 2 to 6 weeks). The serum iron level drawn at 4 to 6 hours drives treatment: desferrioxamine 15 mg per kg per hour intravenous chelation for any symptomatic patient or a level over 350 mcg per dL (60 micromol per L), continued until the patient is clinically well and the level is falling. Whole bowel irrigation with polyethylene glycol is the decontamination of choice for enteric-coated or sustained-release tablets and for a radio-opaque pill mass on abdominal X-ray; activated charcoal does not adsorb iron and has no role. The differential is other heavy metals (lead, arsenic) and the tricyclic antidepressant overdose (wide QRS). ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Related topics
- The toxidrome approach and the general management of the poisoned patient
- Tricyclic antidepressant poisoning (emergency department diagnosis and management)
- Salicylate poisoning
- Paracetamol poisoning
- Acute kidney injury
- The sick child and paediatric resuscitation
- Paediatric fever and serious bacterial illness (the febrile child in the emergency department)
Iron poisoning is the prototype of the heavy-metal overdose whose entire toxicity flows from a single pharmacological fact: the human body has no excretory mechanism for free iron. Once ingested iron overwhelms the carrying capacity of transferrin — the iron-binding protein that safely transports ferric iron in plasma — the excess circulates as catalytic free iron, and that free iron drives the free-radical lipid peroxidation that destroys mitochondrial membranes in the liver, the gut mucosa, the myocardium, and the vascular endothelium. The Fellowship candidate must hold the five-stage clinical course in mind as a single coherent narrative, because each stage reflects the same underlying free-iron injury unfolding in a different compartment and at a different pace. The gastrointestinal stage is the corrosive and vasodilatory effect of iron on the gut wall; the quiescent stage is free iron distributing silently into tissues while the superficial gut recovers; the shock stage is vasodilation, capillary leak, and mitochondrial poisoning of the vasculature and the heart; the hepatotoxic stage is centrilobular necrosis from free-radical destruction of hepatic mitochondria; and the late obstructive stage is corrosive scarring of the gut wall. The single intervention that changes the outcome is desferrioxamine chelation of the free iron, and the candidate who reaches for activated charcoal — which does not adsorb iron — or who discharges the patient during the quiescent phase, has failed the topic.[1][2][5]

Definition and classification
Iron poisoning is the systemic toxicity that follows ingestion of a dose of elemental iron sufficient to exceed the binding capacity of transferrin. The crucial unit is the elemental iron dose, not the salt weight, because the three common pharmaceutical preparations carry very different amounts of elemental iron per tablet. Ferrous sulphate 325 mg contains 65 mg of elemental iron (20 per cent); ferrous fumarate 325 mg contains approximately 106 mg of elemental iron (33 per cent); ferrous gluconate 325 mg contains approximately 38 mg of elemental iron (12 per cent). A patient who reports swallowing "fifteen 325 mg tablets" has taken a wildly different elemental load depending on which salt, and the candidate who calculates the dose from the salt weight has made the cardinal error.[2][1]
Toxicity is graded by the elemental iron dose ingested per kilogram. A dose under 20 mg per kg of elemental iron typically produces no or only mild gastrointestinal symptoms. A dose between 20 and 40 mg per kg produces significant gastrointestinal toxicity with the risk of systemic progression. A dose between 40 and 60 mg per kg produces systemic toxicity with shock and hepatotoxicity. A dose above 60 mg per kg is potentially lethal. These thresholds are the basis for the triage decisions in the Manoguerra consensus guideline, and the candidate must be able to convert a reported ingestion into an elemental dose and a risk category.[2]
Ferrous sulphate
- 325 mg tablet = 65 mg elemental iron (20 per cent)
- The commonest toddler-ingested preparation; the maternal prenatal tablet
- Twenty 325 mg tablets = 1300 mg elemental; in a 10 kg toddler = 130 mg/kg — well above the 60 mg/kg lethal threshold
Ferrous fumarate
- 325 mg tablet = approximately 106 mg elemental iron (33 per cent)
- The densest elemental load per tablet — most easily underestimated from the salt weight
- Twenty 325 mg tablets = 2120 mg elemental; in a 10 kg toddler = 212 mg/kg — over three times the lethal threshold
Ferrous gluconate
- 325 mg tablet = approximately 38 mg elemental iron (12 per cent)
- The lowest elemental load per tablet — but still hazardous in overdose
- Twenty 325 mg tablets = 760 mg elemental; in a 10 kg toddler = 76 mg/kg — still above the 60 mg/kg lethal threshold
Carbonyl iron / polysaccharide-iron complex
- Elemental iron in a non-ionic complex with low GI bioavailability
- Lower toxicity per milligram than the ionic ferrous salts, but the Fenton mechanism applies once absorbed
- Still calculate and report the dose in elemental iron; do not assume it is harmless
Epidemiology and risk factors
Iron supplements are a leading cause of unintentional poisoning death in young children, and that epidemiology drove the 1997 United States Food and Drug Administration regulation requiring unit-dose packaging of high-dose iron supplements — a public-health intervention that halved paediatric iron deaths. Before that regulation, iron supplements were the single most common cause of pharmaceutical poisoning death in toddlers, with a cluster of deaths documented in Los Angeles in 1992 to 1993 in which children found and swallowed maternal prenatal iron tablets.[5] The at-risk patient is therefore the toddler with access to a maternal or antenatal iron bottle, and the second high-risk group is the pregnant or recently pregnant adult who has access to a large supply and may ingest iron in deliberate self-harm. Elderly patients with gastric-acid-lowering preparations and sustained-release formulations are a smaller but important group because the slow absorption delays the serum peak and can extend the toxic window.[2][1]
Pathophysiology — free iron, free radicals, and the five-stage course

The entire toxicity of iron poisoning is mechanistic. In health, ingested iron is absorbed in the duodenum, bound to transferrin in plasma, and either used for haemoglobin synthesis or stored as ferritin. The body has no regulated excretory route for iron, so all iron homeostasis is managed at the level of absorption. When a toxic dose overwhelms transferrin's binding capacity — the total iron-binding capacity is approximately 50 to 70 micromol per litre — the excess circulates as free iron (Fe2+ and Fe3+), and it is this free iron that is the toxin.[1]
Free iron is a potent catalyst of free-radical lipid peroxidation through the Fenton reaction: free iron reacts with hydrogen peroxide to generate the hydroxyl radical, the most reactive of the reactive oxygen species, which attacks polyunsaturated fatty acids in cell and mitochondrial membranes. The cascade — lipid peroxidation, membrane destruction, mitochondrial failure, ATP depletion, cell death — proceeds fastest in tissues with high metabolic demand and high mitochondrial density, which is why the liver (centrilobular hepatocytes, rich in mitochondria and cytochrome P450), the gut mucosa, the myocardium, and the vascular endothelium bear the brunt.[1]
Three additional mechanisms complete the picture. Direct corrosive injury to the gastrointestinal mucosa produces the early nausea, vomiting, haematemesis, and diarrhoea, and sets up the late scarring that causes pyloric or intestinal stricture. Vasodilation and increased capillary permeability from free-iron-mediated endothelial injury produce the distributive shock of stage three, compounded by third-space losses into the damaged gut and by myocardial depression from mitochondrial poisoning of the cardiomyocyte. Mitochondrial poisoning of hepatocytes with free-radical destruction of the mitochondrial membrane produces the centrilobular (zone 3) hepatic necrosis of stage four, the dominant cause of mortality. The five clinical stages are simply these mechanisms unfolding at their characteristic pace.[1][2]
[1]Clinical presentation — the five stages
The five-stage course is the exam centrepiece, and the candidate must be able to name each stage, its timing, its mechanism, and its clinical features, because the timing of presentation determines the interpretation of the serum iron level and the decision to chelate. The stages overlap in the severely poisoned patient, and a patient who arrives in stage one may progress through all five over the following days.[1][2]
The five stages of iron poisoning
Stage one — the gastrointestinal stage (0 to 6 hours). The earliest and most consistent features are gastrointestinal and reflect both the direct corrosive effect of iron tablets on the gastric and duodenal mucosa and the venodilation produced by circulating free iron. Nausea, vomiting, and diarrhoea are near-universal in a significant ingestion, and the vomitus and stool are frequently bloody — haematemesis and melaena — from mucosal erosion. Abdominal pain is common. A patient who is vomiting blood within a few hours of an iron ingestion is systemically poisoned until proven otherwise. The stage resolves as the gastric tablets pass and the mucosa begins to heal, which is the setup for the deceptive stage two.[1][2]
Stage two — the quiescent stage (6 to 24 hours). This is the lethal trap of iron poisoning and the single highest-yield concept in the topic. The patient looks improved: the vomiting settles, the vital signs may normalise, the abdomen is less tender. The mistake is to read this as recovery and to discharge. What is actually happening is that free iron is distributing out of the plasma and into the tissues — most critically into the hepatic mitochondria — and the superficial gastrointestinal mucosa has healed enough for the symptoms to abate while the mitochondrial injury accumulates. Within hours the patient tips into stage three shock or stage four hepatotoxicity. A patient who appears to recover 6 to 24 hours after a significant iron ingestion is not safe to discharge; observation, a serum iron level, and an anion gap are mandatory.[1][2]
[1]Stage three — the shock stage (12 to 24 hours, may overlap with stage two). Distributive shock emerges as free-iron-mediated endothelial injury produces vasodilation and capillary leak, compounded by third-space losses into the damaged gut, by direct myocardial depression from mitochondrial poisoning of the cardiomyocyte, and by coagulopathy-driven gastrointestinal bleeding. The patient is tachycardic, hypotensive, oliguric, and acidotic — a high-anion-gap metabolic acidosis from lactate (shock-driven) and from the mitochondrial poisoning itself. Coagulopathy from hepatic synthetic failure and from direct inhibition of coagulation factors appears, and altered consciousness, seizures, and coma mark severe CNS free-iron injury. This stage carries the early mortality.[1]
Stage four — the hepatotoxicity stage (1 to 3 days, peak day two). The defining feature is centrilobular (zone 3) hepatic necrosis from free-radical destruction of hepatocyte mitochondria — the liver is the target because portal venous blood delivers the highest free-iron concentration and because centrilobular hepatocytes are rich in mitochondria and cytochrome P450, the very enzymes that amplify the free-radical cascade. Serum aminotransferases rise into the thousands, the international normalised ratio climbs as synthetic function fails, and the patient develops the stigmata of acute liver failure — encephalopathy, hypoglycaemia, and jaundice. Hepatic failure is the dominant cause of iron-poisoning mortality, and a patient who survives stage three may still die in stage four from fulminant hepatic failure. A liver transplant has been the salvage therapy for the patient with irreversible hepatic failure.[1][2]
Stage five — the gastrointestinal obstruction stage (2 to 6 weeks). The corrosive injury of stage one heals by scarring, and in the survivors the late complication is pyloric stenosis or intestinal stricture presenting weeks later with vomiting, early satiety, or subacute bowel obstruction. The candidate who focuses only on the acute presentation and forgets stage five misses the long-term morbidity, and any patient discharged after a significant iron ingestion needs a clear safety-net for late obstructive symptoms.[1][2]
Differential diagnosis
The differential of iron poisoning splits into the mimics of the early gastrointestinal presentation (the corrosive-mucosal-injury picture with vomiting and bleeding), the mimics of the shock-with-acidosis picture, and the mimics of the hepatotoxic picture. The highest-yield distinction for the Fellowship examiner is between iron and the other heavy metals and between iron and the tricyclic antidepressant overdose, because the management diverges sharply.[2]
Iron poisoning
- Five-stage course: GI bleed, quiescent, shock, hepatotoxicity, late stricture
- Toddler access to ferrous sulphate/fumarate; antenatal patient; reported tablet ingestion
- Serum iron over 350 mcg/dL (60 micromol/L); anion-gap metabolic acidosis; leucocytosis; AST/ALT in thousands in stage 4
- Desferrioxamine 15 mg/kg/h IV; whole bowel irrigation for enteric-coated/radio-opaque pills; charcoal useless
Tricyclic antidepressant
- Anticholinergic toxidrome (dry, hot, dilated, drowsy) plus cardiovascular toxicity
- Reported amitriptyline/nortriptyline ingestion; rapid onset within 1 to 2 hours
- ECG QRS over 100 ms, right-axis deviation of the terminal R wave in aVR, QT prolongation; iron level normal
- Intravenous sodium bicarbonate for QRS widening and arrhythmia; hyperventilate to pH 7.45 to 7.55; avoid class Ia/Ic antiarrhythmics
Lead poisoning
- Chronic, insidious encephalopathy, abdominal pain, constipation, microcytic anaemia
- Industrial, pica, retained bullet, Ayurvedic or cosmetic exposure over weeks to months
- Whole-blood lead level raised; basophilic stippling; gum lead line; iron level normal
- Chelation with succimer (DMSA), EDTA, or dimercaprol depending on severity and encephalopathy
Arsenic poisoning
- Severe gastroenteritis with rice-water diarrhoea, cardiogenic shock, garlic breath, QT prolongation
- Acute ingestion or chronic exposure (contaminated water, pesticide, homicidal)
- 24-hour urine arsenic raised; iron level normal; sensorimotor neuropathy in survivors
- Chelation with dimercaprol (BAL) then succimer; supportive care for shock and arrhythmia
Salicylate poisoning
- Tinnitus, hyperventilation, sweating, agitation; mixed respiratory alkalosis and high-AG metabolic acidosis
- Reported aspirin ingestion; chronic salicylism in the elderly
- Serum salicylate raised; iron level normal; the mixed acid-base disorder is the discriminator
- Sodium bicarbonate urinary alkalinisation; haemodialysis for severe toxicity
Infectious gastroenteritis
- Vomiting and diarrhoea with fever, typically self-limiting over days
- No access to iron tablets; infectious contact; absence of shock or acidosis
- Iron level normal; leucocytosis less marked; no anion-gap acidosis in the simple case
- Supportive fluids; the danger is misattributing an iron ingestion to gastroenteritis
The hepatotoxic stage mimics paracetamol (acetaminophen) hepatotoxicity — both produce centrilobular necrosis with AST/ALT in the thousands and coagulopathy — and a deliberate self-harm ingestion should always trigger a paracetamol level alongside the iron level, because the two can coexist. Other hepatic mimics include ischaemic hepatitis ("shock liver"), viral hepatitis, and Wilson disease; the serum iron level, the paracetamol level, and the viral and metabolic panel resolve the differential.[2][4]
Bedside assessment
The history establishes the preparation, the elemental iron content per tablet, the number of tablets ingested, the time of ingestion, and the access — the open bottle within the toddler's reach, the antenatal patient's supply, the deliberate self-harm ingestion. The candidate calculates the elemental dose in milligrams per kilogram at the bedside, because that number drives the triage decision in the consensus guideline. A ferrous fumarate ingestion of "twenty tablets" is a very different elemental load from a ferrous gluconate ingestion of the same number, and the patient's weight converts the load into a risk category. Co-ingestants — particularly paracetamol, salicylate, and a tricyclic — are asked for in any deliberate self-harm presentation.[2][1]
The focused examination documents the vital signs for shock (tachycardia, hypotension, tachypnoea from the metabolic acidosis, hypothermia from mitochondrial failure), the hydration and perfusion state (capillary refill, skin temperature, urine output), the abdomen (tenderness, distension, evidence of gastrointestinal bleeding on rectal examination), and the neurological state (conscious level, seizures, coma). The stigmata of anticholinergic or serotonergic co-ingestants are sought. The skin is examined for the flush of free-iron-mediated vasodilation, and the vomitus and stool are inspected for blood.[2]
Investigations
The cornerstone is the serum iron level, drawn at the time of arrival and again at 4 to 6 hours after ingestion, because the serum iron peaks at 2 to 6 hours and the 4- to 6-hour level best reflects the systemic load. A level drawn after 6 to 8 hours may be falsely reassuring, because iron has by then distributed into tissues and the plasma level falls while the tissue injury continues — the same trap as the quiescent phase, expressed in the laboratory. Serial levels every 2 to 4 hours are sent until the level is clearly falling and the patient is clinically well.[1][2]
[1]The accompanying panel serves four purposes. Venous or arterial blood gas screens for the high-anion-gap metabolic acidosis that is the hallmark of systemic free-iron toxicity — the anion gap rises from lactate (shock) and from the mitochondrial poisoning itself, and a worsening base excess is a marker of ongoing tissue injury that supports the decision to chelate. Renal function and electrolytes identify the consequences of shock (acute kidney injury) and the dysnatraemias of third-space loss. Liver function and coagulation track the hepatotoxic stage — the AST and ALT rise into the thousands, the international normalised ratio climbs, and a falling glucose marks hepatic failure. A full blood count shows the leucocytosis and hyperglycaemia that are characteristic of acute iron toxicity and that help distinguish it from simple gastroenteritis. A 12-lead ECG screens for the cardiotoxicity of severe poisoning and for co-ingested cardiotoxins (the wide-QRS tricyclic). An abdominal X-ray is performed in any significant ingestion to look for radio-opaque iron tablets in the stomach or bowel — iron tablets are radiopaque, and a pill mass on the X-ray is an indication for whole bowel irrigation rather than expectant management. Paracetamol and salicylate levels and a beta-human chorionic gonadotropin are sent on any deliberate self-harm ingestion to exclude a co-ingestant.[1][2][4]
The total iron-binding capacity (TIBC) is of historical interest — a transferrin saturation above 100 per cent indicates free iron — but in practice the TIBC lags the clinical course and the serum iron level with the clinical picture is the basis for treatment. The iron-to-TIBC ratio over 1 is a theoretical indicator of free iron but is unreliable in the acute setting.[1]
The ED workup of the suspected iron ingestion
1
2
3
4
5
6
7
8
Immediate management and resuscitation

Resuscitation follows ABCDE with two overriding principles that distinguish iron from every other overdose: there is a specific antidote (desferrioxamine) whose role is to chelate the free iron, and the decontamination of choice is whole bowel irrigation, not activated charcoal.[2][4]
[1]The airway is secured and ventilation established in any patient with reduced consciousness or shock; hypoglycaemia is excluded at the bedside because hepatic failure produces hypoglycaemia in stage four. Intravenous access is established and cardiac monitoring is continuous because severe iron toxicity can produce myocardial depression and arrhythmia. Intravenous crystalloid is given in aliquots (10 to 20 mL per kg boluses of normal saline or balanced crystalloid) to restore intravascular volume in the distributive shock of stage three, titrated to perfusion, blood pressure, and urine output. Blood is cross-matched early in any patient with significant gastrointestinal bleeding. The shock of iron poisoning is distributive and hypovolaemic, and the resuscitation must keep pace with the capillary leak — under-resuscitation allows the metabolic acidosis to deepen and the mitochondrial injury to accelerate.[1][2]
[1]Decontamination is whole bowel irrigation with polyethylene glycol for the patient with enteric-coated or sustained-release tablets or with a radio-opaque pill mass on the abdominal X-ray, on the logic that intact or slow-dissolving tablets continue to deliver iron for many hours and must be flushed mechanically from the gut. Whole bowel irrigation is polyethylene glycol electrolyte solution at 500 mL per hour via nasogastric tube in a child and 1 to 2 L per hour in an adult, continued until the rectal effluent runs clear and the repeat abdominal X-ray shows no residual tablets. The 2023 Tenenbein and Lheureux review in the British Journal of Clinical Pharmacology reaffirms whole bowel irrigation as the decontamination of choice for sustained-release and enteric-coated iron, for packets of iron that form a concretion, and for any radio-opaque pill mass — the indications where activated charcoal fails because the tablets are too large to adsorb and too slow to dissolve.[3][4]
Gastric lavage is considered only for a recent (within one hour), very large, life-threatening ingestion where whole bowel irrigation is not feasible, and only after airway protection; it is not routine and has largely been supplanted by whole bowel irrigation for iron. The 2021 Hoegberg systematic review on activated charcoal confirms that charcoal has no role for iron and other metals, because the metal ion does not adsorb to the charcoal surface.[4]
Definitive management — desferrioxamine chelation
Desferrioxamine (deferoxamine) is the specific antidote. It is a chelating agent — a siderophore analogue — that binds free iron in a stable 1:1 complex called ferrioxamine, which is water-soluble, non-toxic, and excreted in the urine, where it gives the urine the characteristic vin rose (reddish-brown) colour that is the bedside marker of active chelation. By binding the free iron before it reaches the mitochondrion, desferrioxamine interrupts the free-radical cascade at its source.[1][2]
The indications for desferrioxamine are any symptomatic patient — shock, altered consciousness, persistent vomiting, metabolic acidosis — or a serum iron level over 350 mcg per dL (60 micromol per L), with a lower threshold for levels above 500 mcg per dL in some guidelines. The decision is clinical first and biochemical second: a symptomatic patient is chelated regardless of the level, and a high level is chelated regardless of the symptoms. The dose is 15 mg per kg per hour intravenously, begun at a slower rate and titrated up to minimise the infusion-related hypotension that is the commonest side effect; in massive poisoning some toxicology protocols titrate higher under intensive-care monitoring. Therapy continues until the patient is clinically well and the serum iron level is clearly falling — typically 6 to 12 hours, and the infusion is not prolonged beyond 24 hours because prolonged chelation carries its own toxicity.[1][2]
Desferrioxamine (deferoxamine) in iron poisoning
The chelation decision algorithm — who gets desferrioxamine
1
2
3
4
5
6
Three complications of desferrioxamine the candidate must name. Infusion-related hypotension is the commonest and is managed by slowing the rate after ensuring adequate intravascular volume. Acute respiratory distress syndrome (ARDS) complicates prolonged infusions (over 24 hours) and is the reason the infusion is time-limited — the pulmonary toxicity is attributed to the ferrioxamine complex itself or to iron chelated from the pulmonary endothelium. Yersinia enterocolitica sepsis is the feared infective complication, because ferrioxamine acts as a siderophore-like growth factor for Yersinia, which depends on exogenous iron for virulence; any patient on desferrioxamine who develops fever or sepsis is evaluated for Yersinia and treated empirically. Rare anaphylaxis and renal toxicity are also described. The candidate who continues a desferrioxamine infusion for days without a clear endpoint has traded the iron toxicity for desferrioxamine toxicity.[1][2]
Subtypes and scenarios
Enteric-coated and sustained-release ingestion is the acute overdose most likely to be underestimated. The slow-dissolving preparation produces a delayed serum peak — the level drawn at 4 to 6 hours may be low and then climb — and intact tablets may congregate and form a radio-opaque mass on the abdominal X-ray. Whole bowel irrigation is the decontamination of choice for these preparations and for any concretion, and serial iron levels are tracked over 12 to 24 hours because the absorption window is extended. The candidate who discharges a sustained-release ingestion on a single early normal level has missed the delayed peak.[3][2]
Pregnancy deserves a note. Iron crosses the placenta and the fetus is at risk from maternal iron toxicity, particularly in the third trimester. Acute iron poisoning in pregnancy is managed identically — desferrioxamine is not contraindicated in pregnancy and is given on the standard indications, with obstetric and toxicology input. The fetus is monitored, and the threshold to treat is lower because the fetal serum iron may exceed the maternal.[2][5]
The toddler ingestion is the canonical lethal scenario. A single adult ferrous sulphate tablet carries 65 mg of elemental iron, and 60 mg per kg is potentially fatal — a 10 kg toddler needs only about nine tablets to reach the potentially-lethal threshold. Every open bottle within a child's reach is a medical emergency until the count is reconciled, the child is observed, and the serum iron level is confirmed to be safe. The post-1997 unit-dose packaging regulation is the public-health response to the cluster of toddler deaths documented in the 1993 Morbidity and Mortality Weekly Report, and the candidate should be able to cite the regulation and the rationale.[5][2]
Complications and pitfalls
The complications of iron poisoning are the consequences of the free-iron injury and of the chelation. Shock and multi-organ failure are the early causes of death. Fulminant hepatic failure from centrilobular necrosis is the dominant late cause of death and is the indication for which emergency liver transplantation has been used as salvage. Gastrointestinal bleeding from corrosive mucosal injury complicates stage one and stage three. Pyloric stenosis or intestinal stricture from corrosive scarring presents weeks later as stage five. Acute respiratory distress syndrome and Yersinia enterocolitica sepsis are the complications of prolonged desferrioxamine. Acute kidney injury arises from shock and from pigment injury.[1][2]
The pitfalls are well described and the candidate must name them. The first is discharging the patient during the quiescent phase because the vomiting has settled — the lethal trap. The second is giving activated charcoal, which does not adsorb iron, and so delaying the whole bowel irrigation and the chelation. The third is calculating the dose from the salt weight rather than the elemental iron content, underestimating a ferrous fumarate ingestion (33 per cent elemental) and overestimating a ferrous gluconate ingestion (12 per cent elemental). The fourth is interpreting a late-drawn serum iron level as reassuring when free iron has already distributed into tissues. The fifth is continuing a desferrioxamine infusion beyond 24 hours and causing pulmonary toxicity or Yersinia sepsis. The sixth is missing a co-ingested paracetamol dose in a deliberate self-harm presentation and allowing a silent paracetamol hepatotoxicity to evolve alongside the iron injury. The seventh is forgetting the late obstructive stage and failing to safety-net the discharged patient for pyloric stenosis or intestinal stricture at two to six weeks.[1][2][3][4]
Prognosis and disposition
The prognosis depends on the elemental dose, the timing of desferrioxamine, and the development of hepatotoxicity. A patient treated early with chelation before the onset of shock and hepatotoxicity has a good prognosis; a patient who arrives in stage three or stage four has a significant mortality, and fulminant hepatic failure carries the worst outlook. The patient is observed for a minimum of 6 hours from ingestion, and is discharged only if asymptomatic with a normal examination, a normal venous gas with no anion-gap acidosis, and a serum iron level that is clearly falling — never on apparent clinical recovery alone, because of the quiescent-phase trap. The patient managed with desferrioxamine is admitted to a monitored bed, typically intensive care for the patient in shock or with hepatotoxicity. A psychiatric and self-harm risk assessment is begun in any deliberate ingestion once the patient is medically stable, and the late-obstructive safety-net is given at discharge.[1][2]
Special populations
The toddler is the highest-risk group: the dose per kilogram that reaches lethal territory is small, the access to a maternal iron bottle is the usual scenario, and the presentation may be delayed because the ingestion was unwitnessed. A high index of suspicion, an early serum iron level, and a low threshold for observation and chelation govern the management. The pregnant or antenatal patient has a lower threshold to treat because the fetus is at risk, and desferrioxamine is not contraindicated in pregnancy. The elderly patient on a sustained-release preparation has a delayed serum peak that mandates serial levels and a longer observation window. The patient presenting in stage three or four shock or hepatotoxicity is managed in intensive care with desferrioxamine, aggressive fluid resuscitation, correction of coagulopathy and acidosis, and early discussion with a hepatology and liver-transplant service for the patient with fulminant hepatic failure.[2][5][1]
The landmark evidence
The iron-poisoning evidence base is small, consensus-driven, and built on the free-iron and free-radical framework the candidate must be able to cite by author and year. The five papers below are the load-bearing references, and each TrialCard captures the design, the population, and the exam-relevant finding. Memorise the author and the year for each, because the Fellowship viva rewards the candidate who can name the source of the elemental-dose triage threshold (Manoguerra 2005) and the source of the whole-bowel-irrigation indication (Tenenbein and Lheureux 2023). [1]
Toxicokinetics and toxicodynamics of iron poisoning
Toxicology Letters (1998)
PMID 10022330
Narrative expert review
Population: The mechanistic framework for all acute iron ingestions
Key finding
Established the free-iron and free-radical (Fenton-reaction) framework that underpins the five-stage course and the chelation rationale: iron has no excretory route, transferrin saturation releases catalytic free iron, and the free radical drives mitochondrial lipid peroxidation with centrilobular hepatic necrosis. The foundational paper every Fellowship answer is built on.
Iron ingestion — an evidence-based consensus guideline for out-of-hospital management
Clinical Toxicology (2005)
PMID 16255338
Joint EAPCCT/AAPCT consensus guideline
Population: Out-of-hospital triage of iron ingestions
Key finding
Codified the elemental-iron-dose triage thresholds (under 20 mg per kg observe at home, 20 to 40 mg per kg medical evaluation, over 40 mg per kg acute medical care) and the principle that the elemental dose — not the salt weight — drives disposition. The consensus reference for the pre-hospital and ED triage of iron.
The role of whole bowel irrigation in the treatment of toxic ingestions
British Journal of Clinical Pharmacology (2023)
PMID 36639859
Narrative review and position statement
Population: Toxic ingestions amenable to mechanical gut decontamination
Key finding
Reaffirmed whole bowel irrigation with polyethylene glycol as the decontamination of choice for sustained-release and enteric-coated iron, for iron-tablet concretions, and for any radio-opaque pill mass on the abdominal X-ray — precisely the indications where activated charcoal fails. Polyethylene glycol 1 to 2 L per h adult, 500 mL per h child, via nasogastric tube until the effluent clears.
Systematic review on the use of activated charcoal for gastrointestinal decontamination following acute poisoning
Clinical Toxicology (2021)
PMID 34424785
Systematic review and EAPCCT position statement
Population: Poisoned patients considered for charcoal decontamination
Key finding
Confirmed that activated charcoal does not adsorb metal ions and has no role in iron poisoning; charcoal is reserved for organic-molecule ingestions within one hour. For iron the decontamination is whole bowel irrigation, not charcoal.
Toddler deaths resulting from ingestion of iron supplements — Los Angeles, 1992-1993
MMWR Morbidity and Mortality Weekly Report (1993)
PMID 8429817
Surveillance case cluster
Population: Toddlers with access to maternal iron supplements
Key finding
Documented the cluster of paediatric iron-poisoning deaths that drove the 1997 FDA unit-dose packaging regulation and halved US toddler iron deaths. The epidemiological anchor and the public-health rationale for the toddler-access scenario the examiner expects.
Evidence and regional guidelines
The evidence base and the regional practice are well aligned across the Anglosphere. The Manoguerra 2005 consensus guideline (Clinical Toxicology) — the joint European Association of Poison Centres and Clinical Toxicologists and American Academy of Clinical Toxicology out-of-hospital triage guideline — establishes the elemental-iron-dose thresholds for triage (under 20 mg per kg observation at home, 20 to 40 mg per kg medical evaluation, above 40 mg per kg acute medical care) and remains the consensus reference for the pre-hospital and emergency department disposition.[2] The Tenenbein 1998 review (Toxicology Letters) is the foundational toxicokinetic and toxicodynamic paper, establishing the free-iron and free-radical framework that underpins the chelation rationale and the five-stage course.[1] The Tenenbein and Lheureux 2023 review (British Journal of Clinical Pharmacology) reaffirms whole bowel irrigation as the decontamination of choice for sustained-release and enteric-coated iron and for radio-opaque pill masses, with polyethylene glycol at the rates cited above.[3] The Hoegberg 2021 systematic review (Clinical Toxicology) confirms that activated charcoal has no role for iron and other metals.[4] The 1993 Morbidity and Mortality Weekly Report on the Los Angeles toddler deaths is the epidemiological anchor and the driver of the 1997 unit-dose packaging regulation.[5]
ANZ practice note. The Australasian approach follows the integrated pathway: a serum iron level (drawn at 4 to 6 hours) on any symptomatic patient or any significant ingestion, with serial levels every 2 to 4 hours until clearly falling; aggressive intravenous crystalloid for the distributive shock; explicit avoidance of activated charcoal (it does not adsorb iron); whole bowel irrigation with polyethylene glycol (500 mL per hour in a child, 1 to 2 L per hour in an adult, via nasogastric tube, until effluent clears) for enteric-coated or sustained-release tablets and for any radio-opaque pill mass on the abdominal X-ray; and desferrioxamine 15 mg per kg per hour intravenously for any symptomatic patient or a level over 350 mcg per dL (60 micromol per L), continued for 6 to 12 hours and not beyond 24 hours. Discussion with the regional toxicology service (Poisons Information Centre 13 11 26) is the norm for any case meeting chelation criteria, and intensive care plus hepatology for the patient in shock or hepatotoxicity. [1]
SAQ — Adult deliberate self-harm iron overdose: desferrioxamine chelation decision and pharmacology
10 minutes · 10 marks
A 23-year-old woman (62 kg) is brought to the emergency department 90 minutes after a deliberate ingestion of 40 tablets of ferrous fumarate 325 mg with alcohol. She has vomited four times, the vomitus coffee-ground, and has had two episodes of bloody diarrhoea. She is drowsy but reusable, heart rate 124, blood pressure 92/54, capillary refill 4 seconds, respiratory rate 24. Abdominal X-ray shows a cluster of radio-opaque tablets in the stomach. The serum iron drawn at 4 hours is 740 mcg per dL (133 micromol per L). Venous gas: pH 7.24, bicarbonate 14, base excess minus 12, anion gap 24. Lactate 6.2 mmol per litre.
SAQ — The five stages of iron toxicity: the quiescent-phase trap and the late obstructive stage
10 minutes · 10 marks
A 3-year-old boy (14 kg) is brought in 8 hours after a witnessed ingestion of an unknown number of his mother’s ferrous sulphate 325 mg tablets. He vomited twice shortly after the ingestion, including some blood-stained material, but has not vomited for the past 4 hours. He now looks well: alert, playing with a toy, heart rate 110, blood pressure 100/62, capillary refill 2 seconds, afebrile. The mother is asking whether she can take him home. The triage nurse has booked him for discharge.
Exam pearls [1]
- The five stages in one breath: stage one gastrointestinal (nausea, vomiting, haematemesis, diarrhoea, 0 to 6 hours, corrosive mucosal injury), stage two quiescent (apparent recovery, 6 to 24 hours — the lethal trap, free iron distributing into mitochondria), stage three shock (12 to 24 hours, distributive with capillary leak and metabolic acidosis), stage four hepatotoxicity (1 to 3 days, centrilobular necrosis with AST/ALT in thousands, the dominant cause of death), stage five obstruction (2 to 6 weeks, pyloric or intestinal stricture from corrosive scarring).
- The dose unit is elemental iron, not the salt: ferrous sulphate 20 per cent, ferrous fumarate 33 per cent, ferrous gluconate 12 per cent — calculate from the elemental content before triaging.
- Activated charcoal does not adsorb iron; whole bowel irrigation is the decontamination of choice for enteric-coated, sustained-release, or radio-opaque pill mass ingestions.
- Desferrioxamine 15 mg per kg per hour intravenously for any symptomatic patient or a level over 350 mcg per dL (60 micromol per L); vin rose urine is the marker of active chelation; limit to 24 hours to avoid ARDS and Yersinia enterocolitica sepsis.
- The differential is the other heavy metals (lead, arsenic) and the tricyclic antidepressant overdose (wide QRS — give sodium bicarbonate, not desferrioxamine); never discharge on apparent recovery in the quiescent phase.
- The serum iron peak is 2 to 6 hours; the 4- to 6-hour level drives the chelation threshold (over 350 mcg per dL = 60 micromol per L); a level drawn after 6 to 8 hours may be falsely low as iron distributes into tissues — interpret it with the symptoms and the anion gap, never in isolation.
- The high-anion-gap metabolic acidosis is the biochemical signature — lactate from shock plus the mitochondrial poisoning itself; a widening anion gap or a worsening base excess on serial gases is an indication to chelate even when the iron level is equivocal.
- Exchange transfusion (not standard dialysis) is the salvage option for a massive iron level over 1000 mcg per dL or chelation-refractory shock; dialysis does not remove free iron but treats the AKI and the refractory acidosis. [1]
Model answer — A 19-month-old, 12 kg boy is brought to the emergency department one hour after his mother found him with an open bottle of her ferrous sulphate 325 mg tablets. He has vomited three times, the vomitus coffee-ground in colour, and is lethargic and tachycardic at 150, blood pressure 88/52, capillary refill 3 seconds. Abdominal X-ray shows a cluster of radio-opaque tablets in the stomach. Serum iron drawn at 4 hours is 620 mcg per dL (111 micromol per L). Venous gas: pH 7.28, bicarbonate 16, base excess minus 8, anion gap 22. Outline the immediate management.
Immediate management. This is significant acute iron poisoning with early systemic toxicity (shock, metabolic acidosis, a level well above 350 mcg per dL). Ferrous sulphate 325 mg contains 65 mg of elemental iron; even a modest number of tablets reaches the potentially-lethal 60 mg per kg threshold in a 12 kg toddler. The level of 620 mcg per dL with the anion-gap metabolic acidosis and the borderline shock meets both clinical and biochemical criteria for desferrioxamine. [1]
Resuscitate in parallel. Airway and breathing — high-flow oxygen, continuous cardiac monitoring, waveform capnography, intravenous access. Circulation — intravenous normal saline 10 to 20 mL per kg boluses titrated to perfusion, blood pressure, and urine output; cross-match blood for the coffee-ground vomitus. Decontamination — whole bowel irrigation with polyethylene glycol 500 mL per hour via nasogastric tube (this is a 19-month-old) until the rectal effluent runs clear and the repeat abdominal X-ray shows no residual tablets; the radio-opaque pill mass is the indication. Do not give activated charcoal — it does not adsorb iron.[3][4]
Desferrioxamine 15 mg per kg per hour intravenously, begun at a slower rate and titrated to the full 15 mg per kg per hour while monitoring blood pressure (infusion-related hypotension is the commonest side effect), continued until he is clinically well and the serum iron is clearly falling — typically 6 to 12 hours, and not beyond 24 hours to avoid acute respiratory distress syndrome and Yersinia enterocolitica sepsis. The vin rose (reddish-brown) urine is the bedside marker of active chelation. Serial iron levels every 2 to 4 hours, daily liver function and coagulation (hepatotoxicity peaks at day two), and a paracetamol and salicylate level to exclude a co-ingestant. Admit to intensive care; involve the regional toxicology service (Poisons Information Centre 13 11 26). Counsel the parents on the late (2 to 6 week) risk of pyloric stenosis or intestinal stricture and the safety-net symptoms at discharge.[1][2]
Red flags
[1]References
- [1]Tenenbein M. Toxicokinetics and toxicodynamics of iron poisoning Toxicol Lett, 1998.PMID 10022330
- [2]Manoguerra AS, Erdman AR, Booze LL, Christianson G, Woolf AD, Scharman EJ, et al. Iron ingestion: an evidence-based consensus guideline for out-of-hospital management Clin Toxicol (Phila), 2005.PMID 16255338
- [3]Tenenbein M, Lheureux P. The role of whole bowel irrigation in the treatment of toxic ingestions Br J Clin Pharmacol, 2023.PMID 36639859
- [4]Hoegberg LCG, Iwersen-Bergmann S, Heyerdahl F, Yates C, Hojer J, Stahl D, et al. Systematic review on the use of activated charcoal for gastrointestinal decontamination following acute oral overdose Clin Toxicol (Phila), 2021.PMID 34424785
- [5]Centers for Disease Control and Prevention (CDC). Toddler deaths resulting from ingestion of iron supplements--Los Angeles, 1992-1993 MMWR Morb Mortal Wkly Rep, 1993.PMID 8429817