EM · Procedural & diagnostic ED skills
Paracentesis and thoracentesis in the emergency department
Also known as Ascitic tap · Abdominal paracentesis · Large-volume paracentesis · Pleural tap · Thoracocentesis · Pleural fluid aspiration
Paracentesis and thoracentesis in the ED — the two percutaneous fluid taps the Fellowship candidate performs, teaches and defends. Paracentesis: the diagnostic ascitic tap (the serum-ascites albumin gradient for the portal hypertension distinction, the cell count and the culture for the spontaneous bacterial peritonitis, the cytology) or the therapeutic large-volume paracentesis for the tense cirrhotic ascites, performed 2 cm superior and medial to the anterior superior iliac spine under ultrasound, with the Z-track and the local anaesthetic. Thoracentesis: the diagnostic pleural tap for the Light criteria (the transudate versus the exudate) or the therapeutic drainage, performed posteriorly one rib space below the fluid level under ultrasound. The complications — the bleeding, the bowel perforation and the post-procedure ascitic fluid leak for paracentesis; the pneumothorax, the bleeding and the re-expansion pulmonary oedema for thoracentesis — and the practical safeguards (the ultrasound, the coagulation check, the fluid-volume limits). ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Related topics
- Pleural effusion (the emergency department workup and the Light criteria)
- Lumbar puncture in the emergency department
- Local anaesthesia and topical agents
- Central and arterial line insertion in the emergency department
- Procedural sedation in the emergency department
- Focused Assessment with Sonography in Trauma (FAST and E-FAST)
- Acute abdominal pain — the emergency department approach
Paracentesis and thoracentesis are the two percutaneous fluid taps the Fellowship candidate is expected to perform, teach and defend under examination. Both share the same logic: the percutaneous aspiration of a pathologic fluid collection for the diagnosis (the fluid analysis) or the relief of the symptoms (the therapeutic drainage), with the ultrasound guidance, the sterile technique, the local anaesthetic and the disciplined stepwise approach. The examiner will press three things on each: the indications and the differential that the fluid will resolve (the ascites for the portal hypertension and the spontaneous bacterial peritonitis; the pleural effusion for the transudate versus the exudate), the landmarks and the stepwise technique (the ASIS and the Z-track for paracentesis, the rib-space-below-the-fluid for thoracentesis), and the complications and their immediate rescue (the bowel perforation and the ascitic fluid leak for paracentesis, the pneumothorax and the re-expansion pulmonary oedema for thoracentesis).[3][4]

Definition and indications
Paracentesis is the percutaneous needle aspiration of ascitic fluid from the peritoneal cavity. It is performed for the diagnosis of the new or the worsening ascites, the suspected spontaneous bacterial peritonitis (SBP), or the malignant ascites; and for the therapy of the tense or the refractory ascites (the large-volume paracentesis, the drainage of several litres for the symptomatic relief). The AASLD recommends that every cirrhotic patient with the ascites admitted to the hospital undergoes a diagnostic paracentesis on the admission, and any patient with a new ascites, a worsening ascites, or the clinical features of the SBP (the fever, the abdominal pain, the hepatic encephalopathy, the renal impairment) has the tap without delay.[2]
Thoracentesis is the percutaneous needle aspiration of pleural fluid from the pleural space. It is performed for the diagnosis of the unexplained pleural effusion (the fluid analysis with the Light criteria for the transudate-versus-exudate distinction, the cell count, the culture, the cytology, the pH and the glucose), and for the therapy of the symptomatic large effusion (the dyspnoea relief) or the empyema (the drainage of the frank pus). The BTS pleural disease guideline recommends the diagnostic tap for every unexplained unilateral effusion of more than 10 mm depth on the ultrasound, and the therapeutic tap for the symptomatic effusion.[5]
Contraindications
The absolute contraindications are few. For the paracentesis, an overlying abdominal wall infection (the cellulitis, the abscess) at the intended puncture site, a massively distended bowel (the intestinal obstruction with the bowel loops lying against the abdominal wall), or a non-cooperative patient who cannot hold still are the absolute ones. A severe coagulopathy is a relative contraindication, not an absolute one: the contemporary evidence confirms that the diagnostic paracentesis is safe with an INR up to 2.0 and the platelets over 50 without the routine correction, because the puncture is small, the abdominal wall is compressible, and the major bleeding rate is under 1 per cent; the FFP or the platelet cover is reserved for the markedly abnormal coagulation or the very large-bore catheter.[2][3]
For the thoracentesis, the overlying chest wall infection, the suspected empyema with a loculated collection that needs a chest drain (rather than a needle tap), and the uncooperative patient with a cough that brings the pleura against the needle are the absolute contraindications. The coagulopathy carries a higher bleeding risk than for the paracentesis because the intercostal vessels are not compressible and the hemothorax can be significant; the BTS advises a careful risk-benefit balance for the INR above 1.5 or the platelets under 50, with the correction considered for the diagnostic tap and the mandatory correction for the therapeutic tap in the coagulopathic patient. A very small effusion (under 10 to 15 mm on the ultrasound, or the no-safe-fluid-window on the ultrasound) is a relative contraindication — the tap is unsafe, the chest drain or the watchful waiting is the alternative.[5]
[1]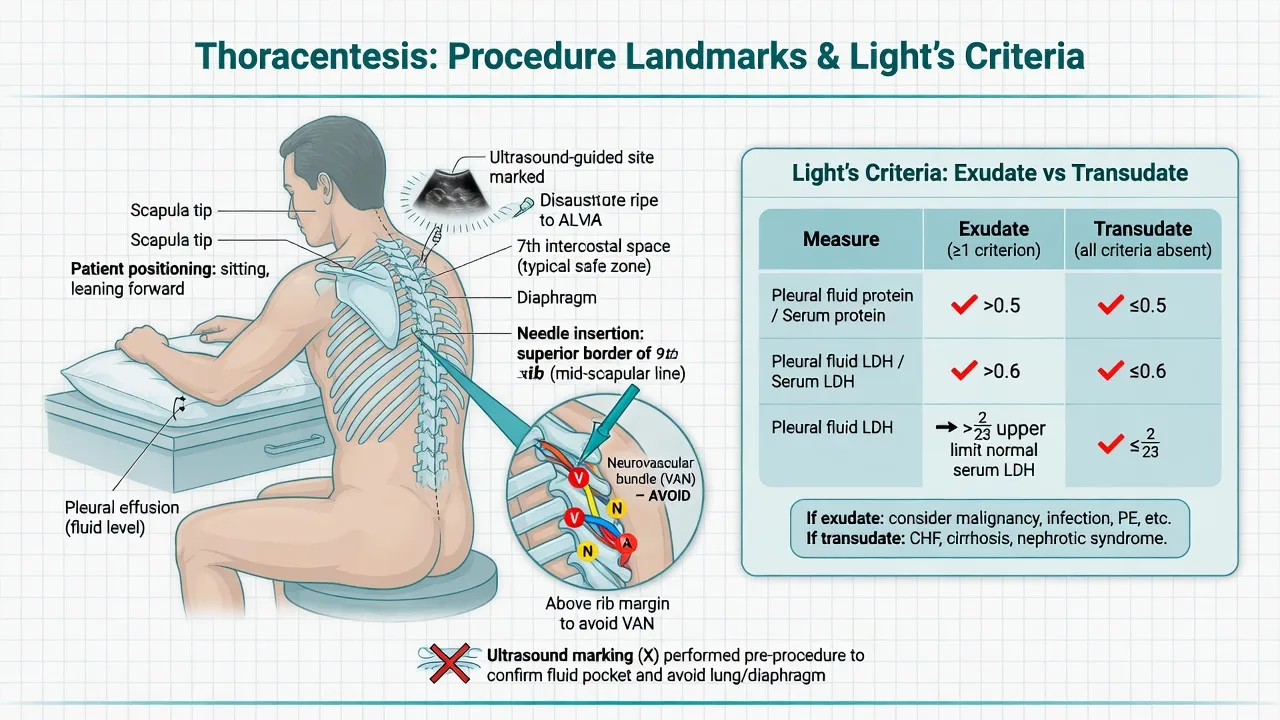
Relevant anatomy and landmarks
The paracentesis site is the left or the right lower quadrant. The safe landmark is 2 cm superior and medial to the anterior superior iliac spine (ASIS), in the left lower quadrant (the left is preferred — the caecum on the right is fixed and gas-filled, the sigmoid on the left is mobile and empties with the patient's positioning). The alternative is the midline 2 cm below the umbilicus in the linea alba, used when the left lower quadrant is scarred or the ultrasound shows no safe window. The ultrasound confirms the depth of the fluid pocket, the absence of the bowel between the abdominal wall and the fluid, and the safe trajectory. The abdominal wall is thinnest at the linea alba and at the ASIS, and the inferior epigastric vessels run along the posterior rectus sheath — the lateral approach away from the midline and away from the rectus muscle avoids them. [1]
The thoracentesis site is the posterior chest, where the dependent fluid collects in the seated patient. The landmark is the upper border of the rib below the fluid level, one to two intercostal spaces below the top of the effusion — never at the top of the effusion (the lung comes down as the fluid drains, and a tap at the top risks the pneumothorax). The needle is advanced over the upper border of the lower rib, avoiding the neurovascular bundle that runs along the lower border of each rib (the V-A-N — vein, artery, nerve — in the costal groove). The ultrasound, performed in the same seated position the tap will be done, marks the level of the fluid, the depth, and the safe interspace; the BTS standard is the real-time ultrasound-guided thoracentesis.[4][5][8]
Equipment
The paracentesis tray contains a ring clamp or a haemostat to stabilise the catheter at the abdominal wall (the catheter can kink or dislodge with the bowel movement), a multiple-hole catheter-over-needle (typically 18 to 20 gauge, 8 to 10 cm long) for the therapeutic drainage, a 20 to 22 gauge spinal needle for the diagnostic tap, lidocaine 1 per cent with a 25G needle for the skin wheal and a longer needle for the deeper infiltration, the syringes (5 mL for the local anaesthetic, 30 to 60 mL for the diagnostic collection), the sterile collection tubes (the aerobic and anaerobic blood culture bottles inoculated at the bedside, the EDTA tube for the cell count, the plain tube for the protein and the albumin and the amylase, the cytology container), the drainage bag for the large-volume paracentesis, the sterile gloves, gown, drape, the chlorhexidine or povidone-iodine, the gauze and the dressing, and the sharps container.[3]
The thoracentesis tray contains a catheter-over-needle (typically 16 to 18 gauge, 6 to 8 cm long) or the needle-catheter assembly for the therapeutic drainage, a 20 to 22 gauge needle for the diagnostic tap, lidocaine 1 per cent, the three-way stopcock and the collection bag or the vacuum bottle, the self-sealing valve to keep the system closed (the air entry prevention), the collection tubes (the heparinised syringe for the pH and the gas analysis, the plain tube for the protein and the LDH and the glucose, the EDTA for the cell count, the culture bottles, the cytology container), the sterile gloves, gown, drape, the chlorhexidine, the gauze and the dressing, and the sharps container. The post-thoracentesis chest X-ray is not routinely required after the ultrasound-guided uncomplicated tap, but is performed for the symptomatic patient, the air aspiration, or the difficult procedure.[4][5]
Patient preparation and consent
The consent is the discussion of the indication, the alternatives (the watchful waiting, the chest drain for the empyema, the diuretic for the heart-failure transudate), the common complications (the pain, the bleeding, the infection, the bowel injury for the paracentesis; the pneumothorax, the bleeding, the re-expansion pulmonary oedema for the thoracentesis), and the post-procedure care. The consent is documented; in the emergency or the encephalopathic patient, the procedure is performed under the emergency exception and the consent is documented after. [1]
The positioning is critical for both procedures. For the paracentesis the patient is placed supine with the head elevated 20 to 30 degrees, the bladder emptied (the catheterisation if the patient is unable to void, to avoid the bladder injury). The ultrasound is performed in the same position the tap will be done, marking the deepest pocket of the fluid (the dependent lower quadrant), the distance from the skin to the fluid, and the absence of the bowel in the trajectory. For the thoracentesis the patient is placed seated upright, leaning forward over a bedside table with the arms resting on the pillows — the position that opens the intercostal spaces and brings the dependent fluid posteriorly. The ultrasound confirms the level of the fluid (the top of the effusion, marked on the skin), the depth, and the safe interspace. The patient who cannot sit is tapped in the lateral decubitus position with the effusion side down, under the ultrasound.[3][4]
The coagulation is checked (the INR, the platelets), the anticoagulant and the antiplatelet therapy are noted — the prophylactic low-molecular-weight heparin is held for one dose where feasible, the therapeutic anticoagulant is managed by the site choice and the post-procedure observation rather than the routine reversal (the bleeding rate is low). The skin is prepped with the chlorhexidine, the full sterile barrier is used (the cap, the mask, the sterile gown, the sterile gloves, the sterile drape), and the time-out is performed before the puncture. [1]
Stepwise technique — the paracentesis
The paracentesis is run to a sequence so that no element is missed. [1]
The paracentesis, in order
- Position and identify. Supine, head elevated 20 to 30 degrees, the bladder emptied. Perform the ultrasound in the same position — mark the deepest fluid pocket, the depth from the skin, and the absence of the bowel in the trajectory. Mark the left lower quadrant, 2 cm superior and medial to the ASIS (or the midline 2 cm below the umbilicus).
- Prep and drape. The chlorhexidine skin preparation, the full sterile barrier (cap, mask, gown, gloves, sterile drape). The time-out: the patient, the side, the indication.
- Anaesthetise. Raise a skin wheal with lidocaine 1 per cent (25G needle, the maximum 3 mg per kilogram plain or 7 mg per kilogram with adrenaline). Infiltrate deeper along the intended track, directing the needle towards the fluid pocket, aspirating before each aliquot, until the ascitic fluid is aspirated.
- The Z-track. Pull the skin 2 to 3 cm caudally with the non-dominant hand, and hold it there while the needle is advanced through the anaesthetised track. The skin returns to its position as the needle is withdrawn, and the offset track seals the puncture — this prevents the persistent ascitic fluid leak. The Z-track is mandatory, not optional.
- Advance the needle or the catheter. Insert the needle (20 to 22 gauge for the diagnostic tap) or the catheter-over-needle (18 to 20 gauge for the therapeutic drainage) with the Z-track held, angled towards the fluid pocket, advancing slowly and steadily. The "pop" or the give is felt as the peritoneum is entered, and the ascitic fluid appears in the hub.
- Collect the diagnostic samples. For the diagnostic tap, aspirate 30 to 60 mL into the syringe and distribute into the culture bottles (the first — inoculate 10 mL into the aerobic and 10 mL into the anaerobic blood culture bottles, the culture yield is doubled over the agar swab), the EDTA tube (the cell count, the absolute neutrophil count), the plain tube (the protein, the albumin for the SAAG, the amylase if the pancreatic source is suspected), and the cytology (the 50 to 100 mL for the highest yield in the suspected malignancy).
- Drain the therapeutic volume. For the large-volume paracentesis, attach the catheter to the drainage bag, secure the catheter at the skin with the suture or the adhesive dressing, and let the fluid drain by gravity. The drainage of 5 to 10 litres is feasible over 1 to 2 hours; the albumin replacement — 8 to 10 g of the 25 per cent albumin per litre drained above 5 litres — is given to prevent the paracentesis-induced circulatory dysfunction and the renal impairment. Stop the drainage at the patient's comfort, the dizziness, or the hypotension.
- Withdraw and dress. Remove the catheter with the Z-track released, apply firm pressure for 2 to 3 minutes, and dress the site with the sterile adhesive. Document the indication, the site, the volume drained, the appearance of the fluid, the samples sent, and the complications. [1]
The two structural errors are to omit the Z-track (the persistent ascitic fluid leak that soaks the dressing and the bed) and to omit the albumin replacement for the large-volume drainage (the paracentesis-induced circulatory dysfunction that precipitates the hepatorenal syndrome in the cirrhotic).[2][7]
Stepwise technique — the thoracentesis
The thoracentesis follows a parallel sequence, with the chest-specific safeguards. [1]
The thoracentesis, in order
- Position and identify. Seated upright, leaning forward over the bedside table with the arms on the pillows (or the lateral decubitus, effusion side down, for the patient who cannot sit). Perform the ultrasound in the same position — mark the top of the effusion on the skin, the depth from the skin to the fluid, and the safe interspace (one to two spaces below the top of the effusion).
- Prep and drape. The chlorhexidine skin preparation, the full sterile barrier (cap, mask, gown, gloves, sterile drape). The time-out: the patient, the side, the indication.
- Anaesthetise. Raise a skin wheal with lidocaine 1 per cent (25G needle, 3 mg per kilogram plain). Infiltrate deeper along the intended track, walking the needle over the upper border of the lower rib (away from the neurovascular bundle in the costal groove), aspirating before each aliquot, until the pleural fluid is aspirated — the anaesthetic track IS the needle track.
- Advance the needle or the catheter. Insert the needle (20 to 22 gauge for the diagnostic tap) or the catheter-over-needle (16 to 18 gauge for the therapeutic drainage) with the same trajectory, walking over the upper border of the lower rib, advancing slowly until the pleural fluid appears. For the therapeutic drainage, advance the catheter over the needle into the pleural space and withdraw the needle — keep the catheter in place with the dominant hand.
- Collect the diagnostic samples. For the diagnostic tap, aspirate 30 to 50 mL into the syringe and distribute into the heparinised syringe (the pH and the gas analysis, sent on ice — under 7.2 suggests the empyema or the malignancy), the plain tube (the protein and the LDH for the Light criteria, the glucose — under 3.3 mmol per litre suggests the empyema or the rheumatoid), the EDTA tube (the cell count and the differential), the culture bottles (inoculated at the bedside), and the cytology (the highest yield in the suspected malignancy). Send the amylase if the pancreatitis or the oesophageal rupture is suspected, and the triglyceride if the chylothorax is suspected (over 1.1 mmol per litre).
- Drain the therapeutic volume. Attach the catheter to the three-way stopcock and the collection bag (or the vacuum bottle). Drain slowly — no more than 1.5 litres at one sitting, and stop immediately at the first chest tightness, the cough, the chest pain, or the new dyspnoea — these are the warning signs of the re-expansion pulmonary oedema. The BTS advises the pleural manometry if more than 1.5 litres is to be drained, with the cessation at the first symptom or the pleural pressure drop.
- Withdraw and dress. Remove the catheter smoothly, apply firm pressure for 2 to 3 minutes, and dress the site. The post-procedure chest X-ray is performed only if the air was aspirated (the pneumothorax), the patient is symptomatic, or the procedure was difficult — the routine post-tap X-ray is not required after the uncomplicated ultrasound-guided tap. [1]
The two structural errors are to tap at the top of the effusion (the lung comes down as the fluid drains, and the needle enters the lung — the pneumothorax) and to drain too much, too fast (the re-expansion pulmonary oedema — the rare but lethal complication).[4][6]
Drug doses — the local anaesthetic
The local anaesthetic infiltration is the only drug in the standard paracentesis or the thoracentesis. Lidocaine 1 per cent is the agent, with a maximum dose of 3 mg per kilogram plain (about 20 mL in the 70 kg adult) or 7 mg per kilogram with adrenaline (about 50 mL in the 70 kg adult). The infiltration is performed with a 25G needle for the skin wheal and a longer needle for the deeper track, aspirating before each aliquot to avoid the intravascular injection. For the thoracentesis, the deeper infiltration walks the needle over the upper border of the lower rib, anaesthetising the periosteum and the parietal pleura — the anaesthetic track IS the needle track, and the first aspiration of the pleural fluid confirms the depth. [1]
The albumin replacement is the second drug of the large-volume paracentesis. The AASLD and the consensus recommend 8 to 10 g of the 25 per cent albumin per litre of the ascitic fluid drained above 5 litres (the 6 to 8 g per litre if the drained volume is 5 litres or less and the patient is low-risk). The rationale is the prevention of the paracentesis-induced circulatory dysfunction — the effective hypovolaemia, the activation of the renin-angiotensin-aldosterone system, and the precipitation of the hepatorenal syndrome — the complication that the Sort NEJM trial established the albumin prevents in the SBP, and that the albumin prevents in the large-volume paracentesis by the same mechanism.[2][7]
The antibiotics for the SBP are the third drug of the diagnostic paracentesis, started at once on the diagnosis of the ascitic neutrophil count of 250 per mm cubed or more. The first-line empirical regimen is the third-generation cephalosporin — the cefotaxime 2 g intravenously every 8 hours or the ceftriaxone 2 g intravenously daily for 5 to 7 days, with the albumin 1.5 g per kilogram at the diagnosis and 1 g per kilogram on day 3 to prevent the hepatorenal syndrome and reduce the mortality (the Sort NEJM trial).[7]
Differential diagnosis — the fluid analysis: SAAG and Light's criteria
The fluid analysis is the single most examinable block of the topic, and it answers the differential that brought the patient to the procedure. For the ascites, the serum-ascites albumin gradient (SAAG) — the serum albumin minus the ascitic albumin — separates the portal-hypertensive (high-gradient, at 1.1 g per dL or more) from the non-portal (low-gradient, under 1.1 g per dL) ascites. Runyon's 1992 paper established the SAAG as superior to the old transudate-exudate concept, with the 97 per cent accuracy for the portal hypertension. For the pleural effusion, the Light criteria — the pleural-to-serum protein ratio over 0.5, OR the pleural-to-serum LDH ratio over 0.6, OR the pleural LDH over two-thirds the upper limit of normal — separate the transudate from the exudate.[1][5]
High-SAAG ascites (portal)
- SAAG at 1.1 g per dL or more — the portal hypertension is present (97 per cent accurate)
- Cirrhosis (the commonest — 80 per cent of the ascites), the heart failure, the Budd-Chiari, the hepatic failure
- Treat the cause; drain the tense or the refractory ascites; the SBP prophylaxis if the ascitic protein is under 1.5 g per dL
- A SAAG over 1.1 with a high fluid protein (over 2.5 g per dL) suggests the cardiac ascites
Low-SAAG ascites (non-portal)
- SAAG under 1.1 g per dL — the portal hypertension is excluded
- Peritoneal carcinomatosis (the ovarian, the gastric, the colon), the tuberculous peritonitis, the pancreatic ascites, the nephrotic, the bowel obstruction
- Send the cytology (50 to 100 mL for the highest yield), the ADA, the amylase; the CT and the peritoneal biopsy if non-diagnostic
- The cytology is positive in about 60 to 90 per cent of the carcinomatosis on the first sample, near 100 per cent on three samples
Exudative pleural effusion
- Light criteria — protein ratio over 0.5, OR LDH ratio over 0.6, OR pleural LDH over 2/3 ULN (any one)
- Bacterial pneumonia (the parapneumonic), the malignancy (the lung, the mesothelioma, the metastasis), the pulmonary embolism, the tuberculosis, the autoimmune (the lupus, the rheumatoid)
- Send the pH and the glucose (under 7.2 or under 3.3 mmol per litre = drain), the cell count, the Gram stain and the culture, the cytology
- A pH under 7.2, a glucose under 3.3, or a positive culture defines the complicated parapneumonic effusion — the chest drain
Transudative pleural effusion
- Light criteria all negative — the systemic cause
- Heart failure (the commonest — bilateral), the cirrhosis (the hepatic hydrothorax — right-sided), the nephrotic, the constrictive pericarditis, the hypoalbuminaemia
- Treat the systemic cause; drain only if the dyspnoea is severe
- A heart-failure effusion on the diuretics can be mislabelled as an exudate (the pseudoexudate) — the serum-pleural albumin gradient over 1.2 g per dL corrects it
The discriminating tests the examiner rewards are: the SAAG over 1.1 for the portal hypertension (the cirrhosis, the heart failure, the Budd-Chiari); the SAAG under 1.1 for the non-portal (the peritoneal carcinomatosis, the TB, the pancreatic); the Light criteria for the pleural transudate-versus-exudate; the pleural pH and the glucose for the complicated parapneumonic effusion (under 7.2 or under 3.3 mmol per litre = drain); and the cytology for the malignancy. The ascitic absolute neutrophil count of 250 per mm cubed or more defines the SBP — irrespective of the symptoms or the culture — and the empirical antibiotics and the albumin start at once.[1][2][5]

Complications — procedure-related and disease-related
The complications of the paracentesis divide into the local, the infectious, and the rare-but-serious. The local complications are the pain, the minor bleeding at the site, and the persistent ascitic fluid leak — the leak is the consequence of the omitted Z-track and is managed with the single suture at the puncture site, the ostomy bag if the leak is large, and the surgical review for the leak beyond 48 hours or the peritonitis. The infectious complications are the cellulitis at the site and the iatrogenic SBP — prevented by the sterile technique and the full barrier. The rare-but-serious complications are the major bleeding (the abdominal wall haematoma, the inferior epigastric artery laceration, the haemoperitoneum in the coagulopathic — under 1 per cent), the bowel perforation (the distended or the adherent bowel, presenting with the peritonitis over hours — managed with the IV antibiotics, the imaging, and the surgical review if the peritonitis develops), and the post-paracentesis circulatory dysfunction (the hypovolaemia, the renal impairment, the hepatorenal syndrome after the large-volume drainage — prevented by the albumin).[2][3]
The complications of the thoracentesis are the pneumothorax (1 to 6 per cent, lower with the ultrasound guidance; the iatrogenic from the lung puncture, or the trapped lung preventing the re-expansion), the bleeding (the chest wall haematoma, the intercostal artery laceration in the elderly with the tortuous intercostal vessels, the haemothorax in the coagulopathic), the infection (the cellulitis, the empyema from the contamination), the vasovagal (the cough, the bradycardia, the hypotension on the pleural puncture — managed with the supine positioning and the fluids), and the re-expansion pulmonary oedema — the rare (under 1 per cent) but potentially lethal complication of the rapid re-expansion of the collapsed lung, presenting with the cough, the dyspnoea, the hypoxia, the frothy sputum within 24 hours of the large-volume drainage. The Feller-Kopman series established the risk factors — the large volume drained (over 1.5 litres), the rapid drainage, the chronicity of the collapse, and the negative pleural pressure — and the BTS recommends the cessation at the first symptom, the 1.5-litre limit, and the pleural manometry for the larger drainage.[5][6]
The complications and the rate
Pitfalls and practical tips
The pitfalls invert the discipline. Tapping without the ultrasound when the ultrasound is available — the avoidable bowel injury and the failed tap. Omitting the Z-track in the paracentesis — the persistent ascitic fluid leak that soaks the dressing and the bed. Tapping at the top of the effusion in the thoracentesis — the lung puncture and the pneumothorax as the lung re-expands. Draining more than 1.5 litres of the pleural fluid — the avoidable re-expansion pulmonary oedema. Forgetting the albumin in the large-volume paracentesis — the paracentesis-induced circulatory dysfunction and the hepatorenal syndrome. Sending the ascitic culture on the swab instead of the inoculated blood culture bottle — the halved culture yield and the missed SBP. Not sending the cytology in the suspected malignancy — the missed diagnosis that demands the 50 to 100 mL for the highest yield. Reversing the coagulopathy routinely before the paracentesis — the unnecessary blood-product exposure for the procedure with the under-1-per-cent bleeding rate.[2][5]
The practical tips are the mirror. The ultrasound for every paracentesis and every thoracentesis, marking the fluid pocket, the depth, and the absence of the bowel or the lung in the trajectory. The Z-track for every paracentesis. The 2-cm-superior-and-medial-to-the-ASIS site for the paracentesis, the one-to-two-spaces-below-the-fluid site for the thoracentesis. The lidocaine 1 per cent (3 mg per kilogram plain), aspirating before each aliquot. The inoculated blood culture bottles for the ascitic and the pleural culture. The albumin for the large-volume paracentesis. The 1.5-litre limit for the thoracentesis, with the cessation at the first symptom. The cytology in the 50 to 100 mL container for the suspected malignancy. The conservative management of the bowel perforation unless the peritonitis develops. The post-thoracentesis chest X-ray only if the air was aspirated or the patient is symptomatic.[3][4][8]
Post-procedure care and disposition
After the paracentesis the patient is observed briefly, the vital signs and the puncture site checked, and the dressing inspected for the leak. The diagnostic tap is a same-day procedure — the patient is discharged with the safety-net advice to return for the fever, the abdominal pain, the bleeding or the leak beyond 24 hours. The large-volume paracentesis is observed for the orthostatic hypotension and the renal function — the albumin is given as outlined, the urine output monitored, and the patient discharged when the haemodynamically stable. The underlying condition determines the disposition — the cirrhotic with the first SBP to the medical ward for the antibiotics and the consideration of the secondary prophylaxis (the norfloxacin 400 mg daily), the malignant ascites to the oncology or the palliative pathway. [1]
After the thoracentesis the patient is observed briefly, the vital signs and the oxygenation checked, and the breath sounds compared with the pre-procedure baseline. The post-procedure chest X-ray is performed only if the air was aspirated, the patient is symptomatic, or the procedure was difficult. The diagnostic tap is a same-day procedure. The therapeutic tap is observed for the re-expansion symptoms (the cough, the dyspnoea, the hypoxia) for the first few hours — the patient is discharged when the oxygenation is stable, the breath sounds are improved, and the symptoms have not developed. The underlying condition determines the disposition — the parapneumonic effusion to the medical team for the antibiotics and the drainage of the complicated effusion (the pH under 7.2, the chest drain), the malignant effusion to the oncology or the respiratory pathway for the pleurodesis.[5]
Special populations
The coagulopathic patient (the INR up to 2.5, the platelets over 50) has the paracentesis without the routine correction — the under-1-per-cent bleeding rate justifies the procedure; the FFP or the platelets are reserved for the markedly abnormal coagulation, the renal failure with the uraemic platelet dysfunction, or the very large-bore catheter. The thoracentesis in the coagulopathic patient is approached more cautiously — the intercostal vessels are not compressible, the hemothorax can be significant, and the abnormal coagulation is weighed with the urgency of the diagnostic question. The cirrhotic patient with the first SBP receives the antibiotics and the albumin, the secondary prophylaxis with the norfloxacin, and the work-up for the liver transplant. The malignant-ascites patient benefits from the therapeutic paracentesis for the symptomatic relief, with the cytology sent on the first tap; the long-term management is the indwelling peritoneal catheter (the PleurX) and the palliative oncology. The obese patient needs the ultrasound for the deeper fluid pocket and the longer needle or catheter. The pregnant patient is positioned in the left lateral tilt, the bladder emptied, and the puncture performed by the experienced operator with the ultrasound — the paracentesis is safe in the pregnancy when the indication warrants. The patient on the antiplatelet or the anticoagulant therapy: the aspirin is continued, the clopidogrel is held for 5 to 7 days if feasible for the therapeutic tap, the prophylactic low-molecular-weight heparin is held for one dose, and the therapeutic anticoagulant is managed by the site choice and the observation.[2][5]
Evidence and regional guidelines
The contemporary framework is built on three pillars. The AASLD Practice Guideline for the management of the adult patient with the ascites due to the cirrhosis (Runyon 2013) codified the SAAG, the diagnostic paracentesis on every cirrhotic admission, the large-volume paracentesis with the albumin replacement, and the SBP diagnosis and treatment — the global standard.[2] The British Thoracic Society Guideline for the Pleural Disease (Roberts 2023) is the contemporary standard for the thoracentesis — the ultrasound guidance for the diagnostic and the therapeutic tap, the 1.5-litre limit for the single drainage, the pleural manometry for the larger drainage, the post-tap chest X-ray only for the symptomatic or the air-aspirated, and the fluid-analysis panel with the Light criteria, the pH and the glucose, the cytology and the culture.[5] The Runyon 1992 paper established the SAAG as superior to the transudate-exudate concept for the ascites, with the 97 per cent accuracy for the portal hypertension — the foundational evidence the examiner rewards.[1] The Sort 1999 NEJM trial established the albumin in the SBP to reduce the renal impairment and the mortality, the evidence that extends to the albumin in the large-volume paracentesis by the same mechanism.[7] The Thomsen 2006 NEJM videos codified the stepwise technique for both procedures.[3][4] The Feller-Kopman 2007 series characterised the re-expansion pulmonary oedema and its risk factors.[6] The Sperandeo 2022 series confirmed the safety of the real-time ultrasound-guided thoracentesis.[8]
ANZ practice note. In the Australian and New Zealand emergency departments the paracentesis and the thoracentesis are performed under the real-time ultrasound guidance, with the full sterile barrier, the local anaesthetic (the lidocaine 1 per cent, 3 mg per kilogram plain), and the disciplined stepwise technique. The diagnostic paracentesis is performed on every cirrhotic admission and on every new or worsening ascites; the ascitic fluid is sent for the cell count, the SAAG, the culture (in the inoculated blood culture bottles), and the cytology, and the SBP (the neutrophil count of 250 per mm cubed or more) is treated at once with the cefotaxime 2 g intravenously every 8 hours and the albumin 1.5 g per kilogram. The large-volume paracentesis is replaced with the albumin 8 to 10 g per litre above 5 litres. The thoracentesis follows the BTS framework — the ultrasound guidance, the one-to-two-spaces-below-the-fluid site, the 1.5-litre limit, the cessation at the first symptom, and the post-tap chest X-ray only for the symptomatic or the air-aspirated. The ACEM and the Gastroenterological Society of Australia endorse the structured training, the sterile technique, and the ultrasound guidance as the quality standard. [1]
Exam pearls
- The SAAG over 1.1 g per dL = portal hypertension (the cirrhosis, the heart failure, the Budd-Chiari); under 1.1 = the peritoneal cause (the carcinomatosis, the TB, the pancreatic). The Runyon 1992 evidence, 97 per cent accurate.
- The SBP = the ascitic neutrophil count of 250 per mm cubed or more — the cefotaxime 2 g intravenously every 8 hours and the albumin 1.5 g per kilogram at the diagnosis, 1 g per kilogram on day 3. The Sort 1999 evidence.
- The paracentesis site: 2 cm superior and medial to the ASIS (left preferred) or 2 cm below the umbilicus in the midline — ultrasound for the fluid pocket and the absence of the bowel. The Z-track is mandatory.
- The thoracentesis site: the posterior chest, seated, one to two spaces below the top of the effusion, advanced over the upper border of the lower rib. Never at the top of the effusion.
- The Light criteria: the protein ratio over 0.5, OR the LDH ratio over 0.6, OR the pleural LDH over 2/3 ULN (any one) = exudate. None = transudate.
- The pleural pH under 7.2 or the glucose under 3.3 mmol per litre = drain (the complicated parapneumonic, the empyema, the malignancy).
- The re-expansion pulmonary oedema: drain no more than 1.5 litres at one sitting, stop at the first chest tightness, the cough or the new pain. The Feller-Kopman evidence.
- The albumin 8 to 10 g per litre above 5 litres drained in the large-volume paracentesis — prevents the paracentesis-induced circulatory dysfunction and the hepatorenal syndrome.
- The coagulopathy is a relative, not an absolute, contraindication — the paracentesis is safe with the INR up to 2.0 and the platelets over 50 without the routine correction.
- The ascitic culture: inoculate the blood culture bottles at the bedside — the yield is doubled over the agar swab. [1]
Short answer questions
SAQ — Cirrhotic ascites: the paracentesis technique and the SAAG
10 minutes · 10 marks
A 58-year-old man with known alcohol-related cirrhosis presents to the emergency department with a three-day history of increasing abdominal distension, a low-grade fever and new-onset confusion. His abdomen is tense and dull to percussion. A bedside ultrasound confirms a large ascitic fluid pocket in the left lower quadrant. You plan a diagnostic paracentesis.
SAQ — Post-thoracentesis deterioration: the complications of thoracentesis
10 minutes · 10 marks
A 72-year-old woman undergoes a therapeutic thoracentesis in the emergency department for a large right-sided malignant pleural effusion. During drainage of the second litre of fluid she develops a sudden cough, chest tightness and dyspnoea. Her oxygen saturation falls from 96 to 89 per cent on room air.
Red flags
[1]References
- [1]Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG. The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites Ann Intern Med, 1992.PMID 1616215
- [2]Runyon BA, AASLD Practice Guidelines Committee. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012 Hepatology, 2013.PMID 23463403
- [3]Thomsen TW, Shaffer RW, White B, Setnik GS. Videos in clinical medicine. Paracentesis N Engl J Med, 2006.PMID 17093242
- [4]Thomsen TW, DeLaPena J, Setnik GS. Videos in clinical medicine. Thoracentesis N Engl J Med, 2006.PMID 17035643
- [5]Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease Thorax, 2023.PMID 37553157
- [6]Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A. Large-volume thoracentesis and the risk of reexpansion pulmonary edema Ann Thorac Surg, 2007.PMID 17954079
- [7]Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis N Engl J Med, 1999.PMID 10432325
- [8]Sperandeo M, Rea G, Carnevale V, et al. Effectiveness and Safety of Real-Time Transthoracic Ultrasound-Guided Thoracentesis Diagnostics (Basel), 2022.PMID 35328278